
Head — MCQs

On this page
Ptosis in Horner syndrome is due to the involvement of which muscle?
Ptosis in Horner syndrome is due to paralysis of which muscle?
A pregnant woman presents with fever, retroorbital pain, headache, pulsatile proptosis of the right eye, and tinnitus. BP and fundus were normal. Which of the following structures are involved?
What is the action of the superior oblique muscle?
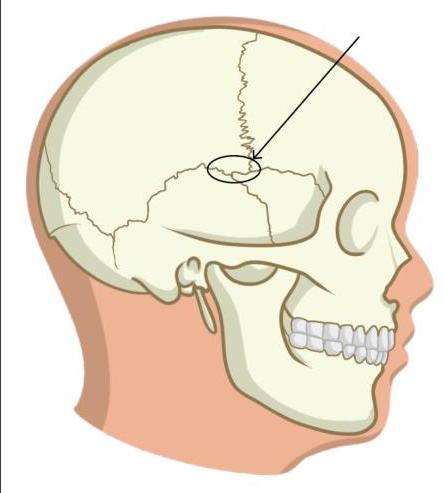
Identify the incorrect statement regarding the marked structure.
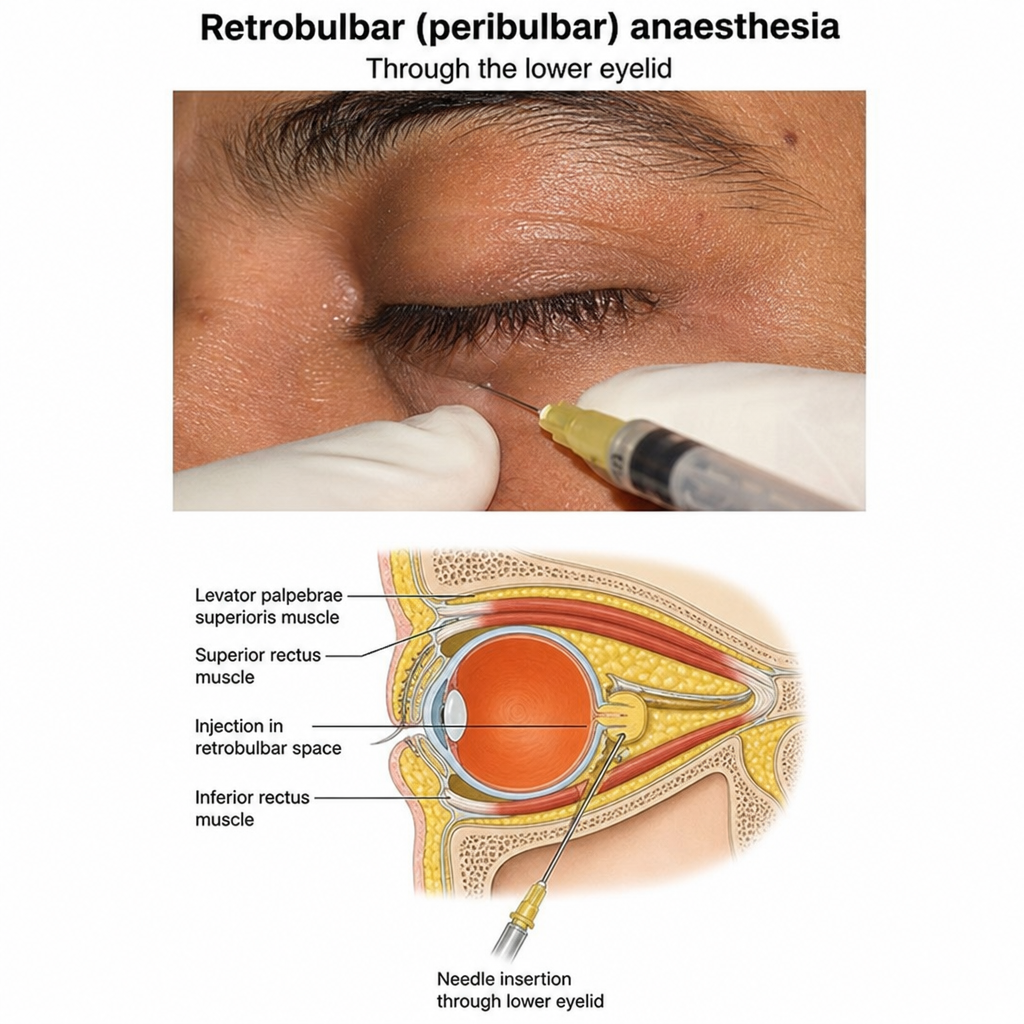
Which regional anesthetic technique is shown in the image given below?
A patient after a road traffic accident presents to the emergency room with difficulty in swallowing and slurred speech. Investigations reveal fractures in the occipitotemporal region. Which of the following areas should be tested in order to find the nerve which is involved?
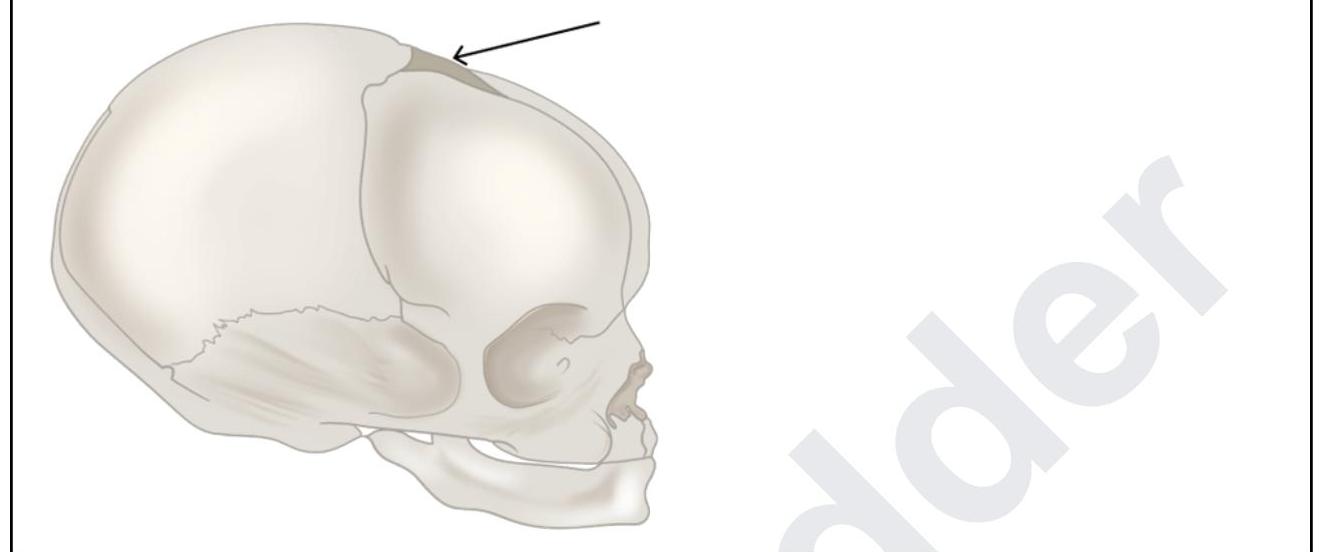
A 6-month-old boy was brought to the casualty with progressive hydrocephalus. The pediatrician performs an anterior fontanelle ventricular tap to obtain CSF. What are the structures punctured by the pediatrician while piercing through the marked structure?
In pediatric assessment, a cephalic index of 75-80 is classified as:
Masseter is supplied by which nerve?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app