
Head — MCQs

On this page
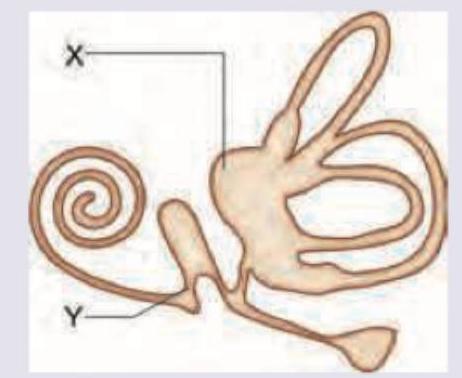
All are correct about the part marked as $X$ and $Y$ except:
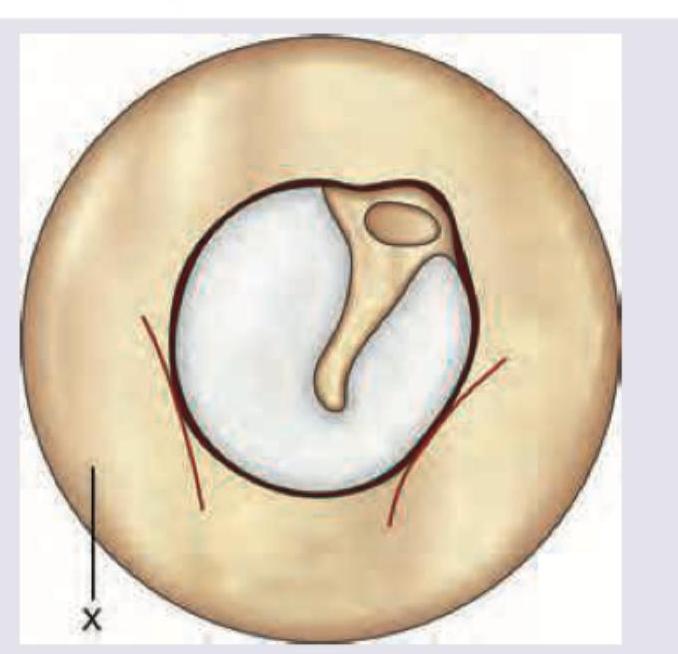
The area of external auditory canal marked as ' $X$ ' is innervated by which nerve?
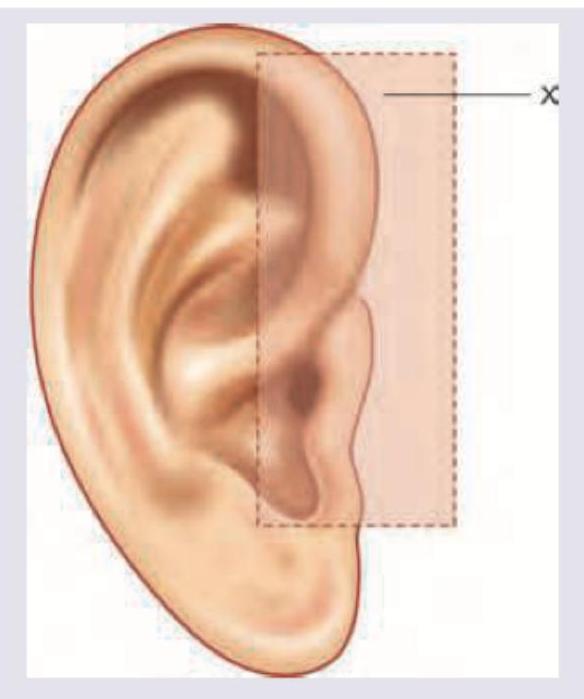
Which of the following nerve supplies the area of pinna marked as X?
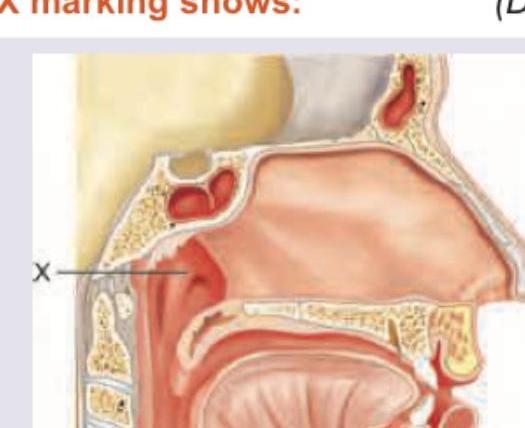
The X marking shows:
In a patient of carcinoma tongue, the infiltration of which muscle causes ankyloglossia ?
All of the following cranial nerves pass through the jugular foramen except :
A fracture of the middle cranial fossa may result in an injury of the
Consider the following statements with reference to scalp : 1. The blood vessels lie within dense connective tissue. 2. The anterior scalp is supplied by supraorbital and supratrochlear vessels. 3. The lateral and posterior scalp is supplied by superficial temporal, posterior auricular and occipital arteries. Which of the statements given above are correct?
Which one of the following statements regarding anatomy of fetal head is NOT true?
Which one of the following cranial nerves does NOT supply the external ear?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app