
Head — MCQs

On this page
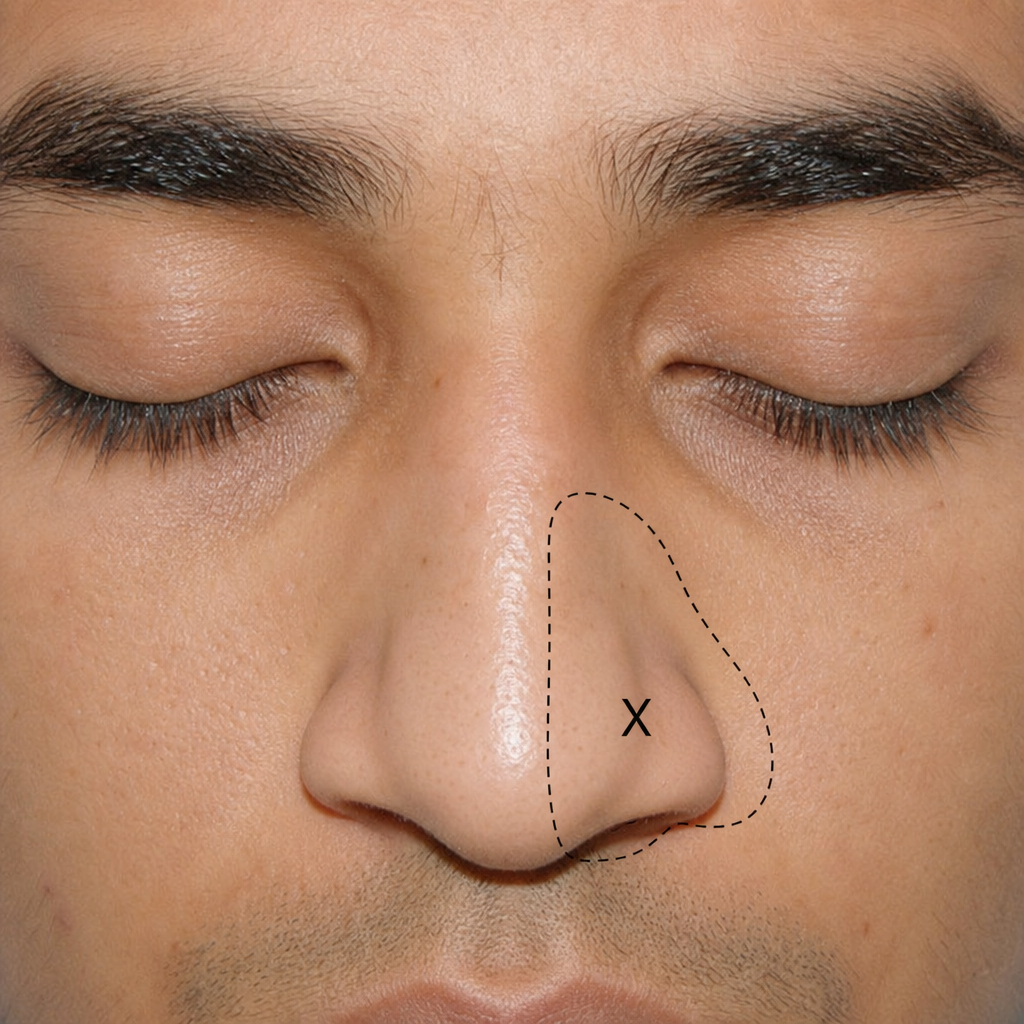
Which nerve supplies the area of nose marked as $X$ ?
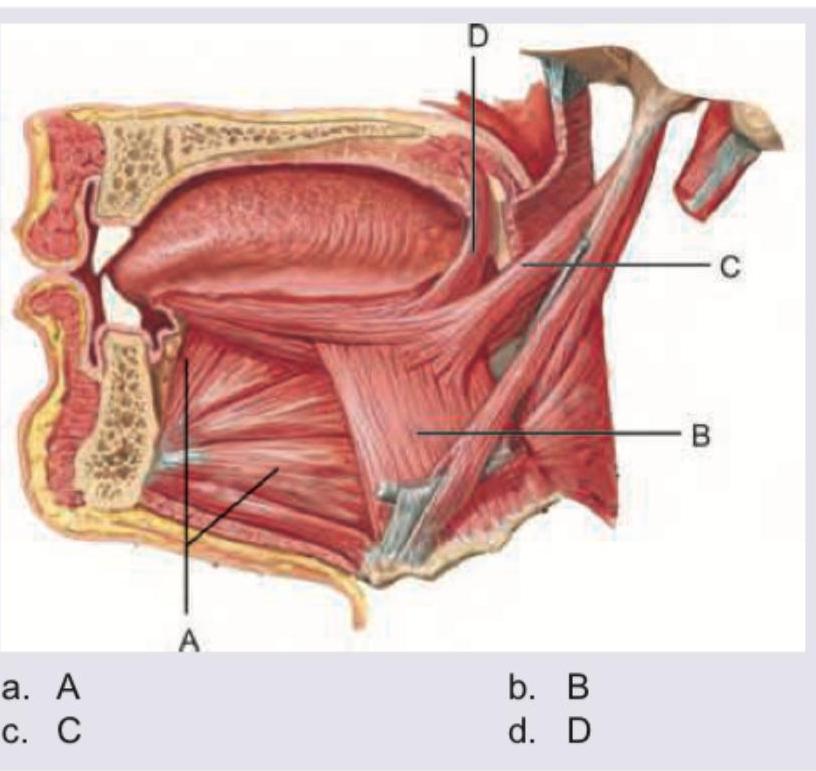
Safety muscle of the tongue is:
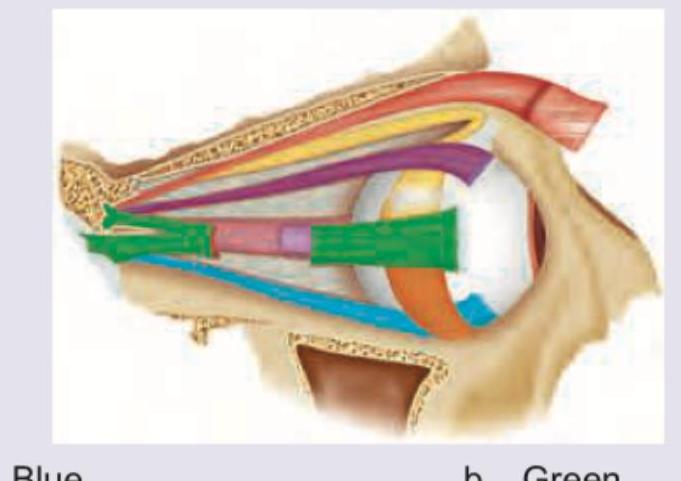
Which of the color-marked muscles shown below is the antagonist muscle to superior rectus?
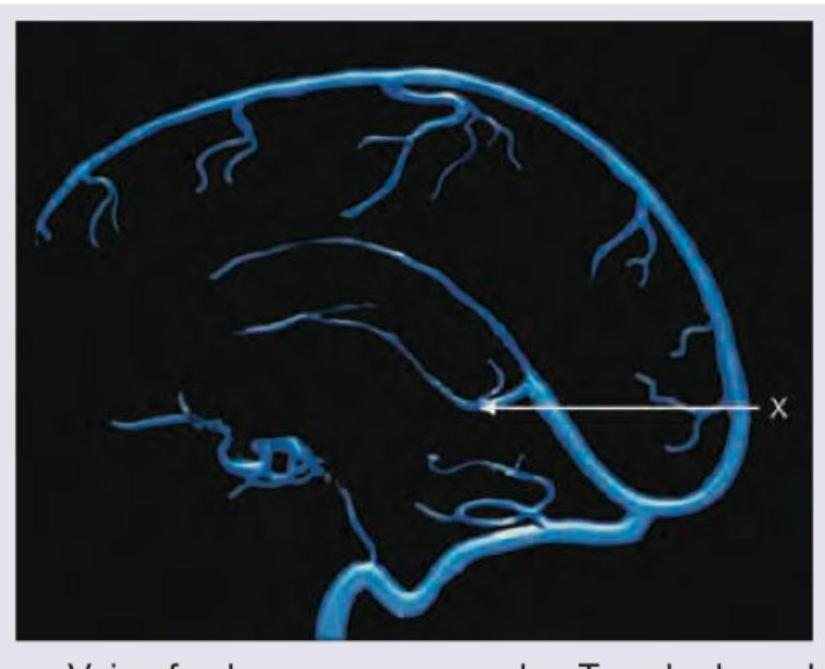
The following structure marked as $X$ is?
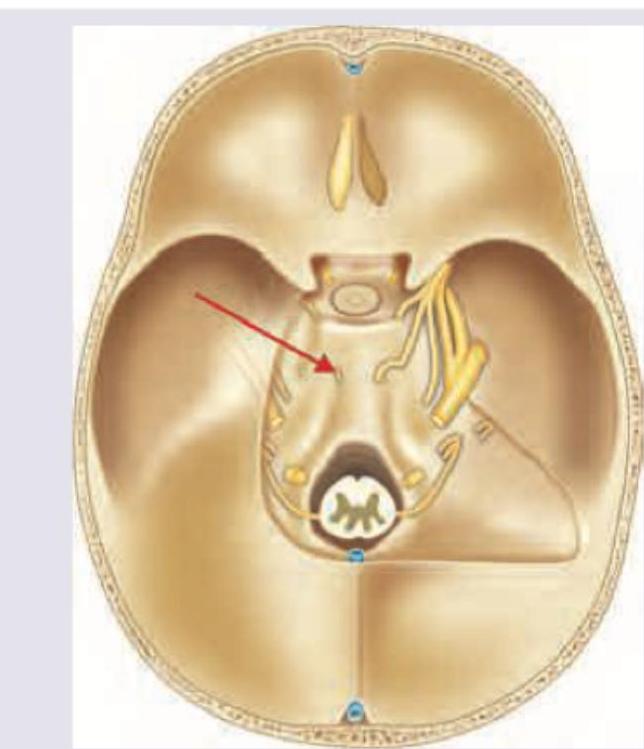
Identify the structure marked by the arrow in this skull base image:
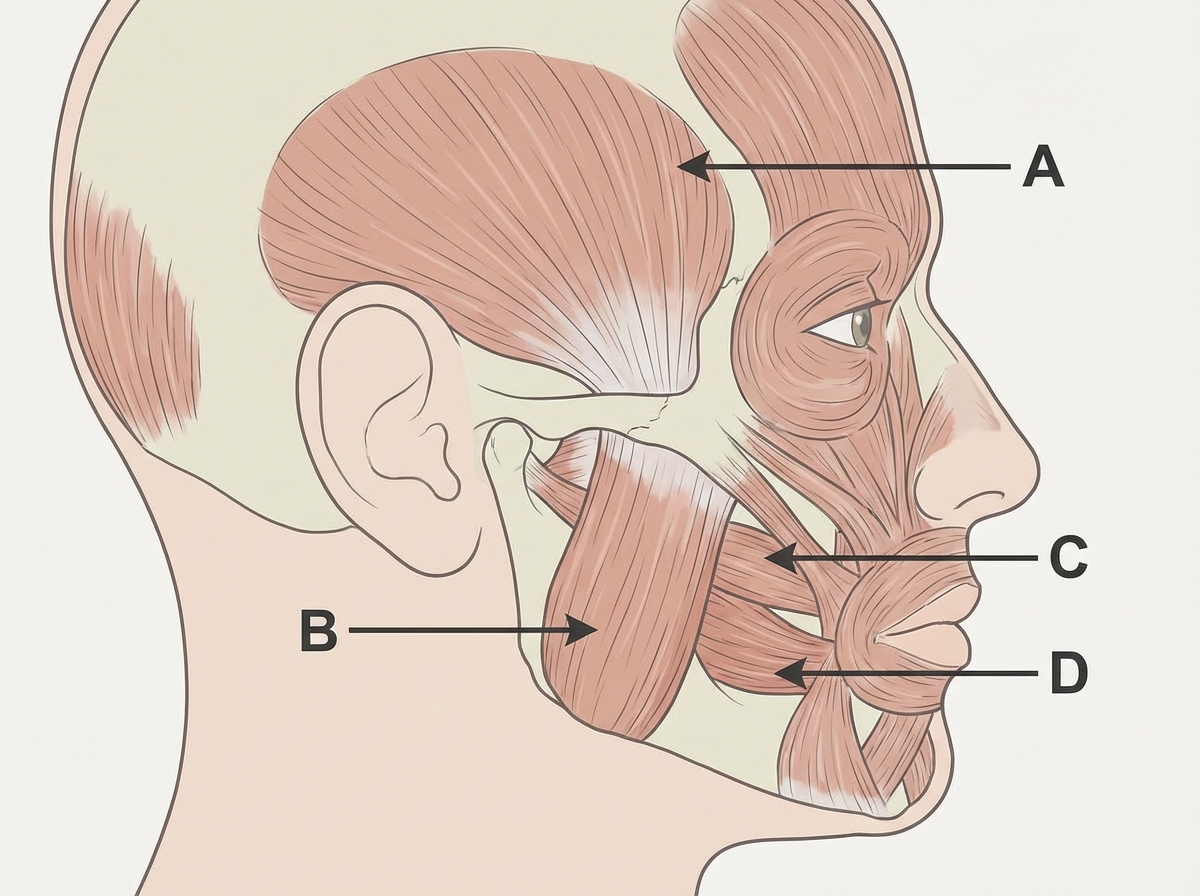
Which of the following structures will help in opening of jaw?
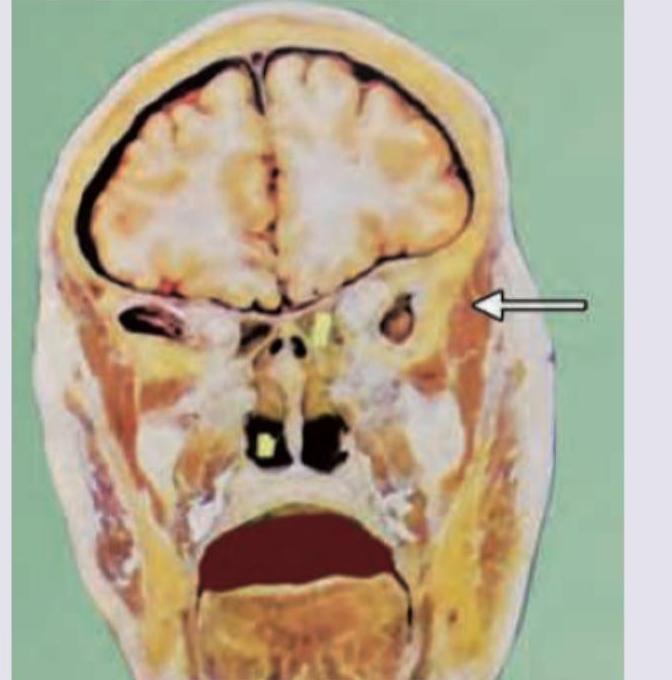
What is the function of the muscle marked in the cut section shown below? (AIIMS May 2018)

Mandibular division of trigeminal nerve passes through which of the following? (AIIMS May 2018)
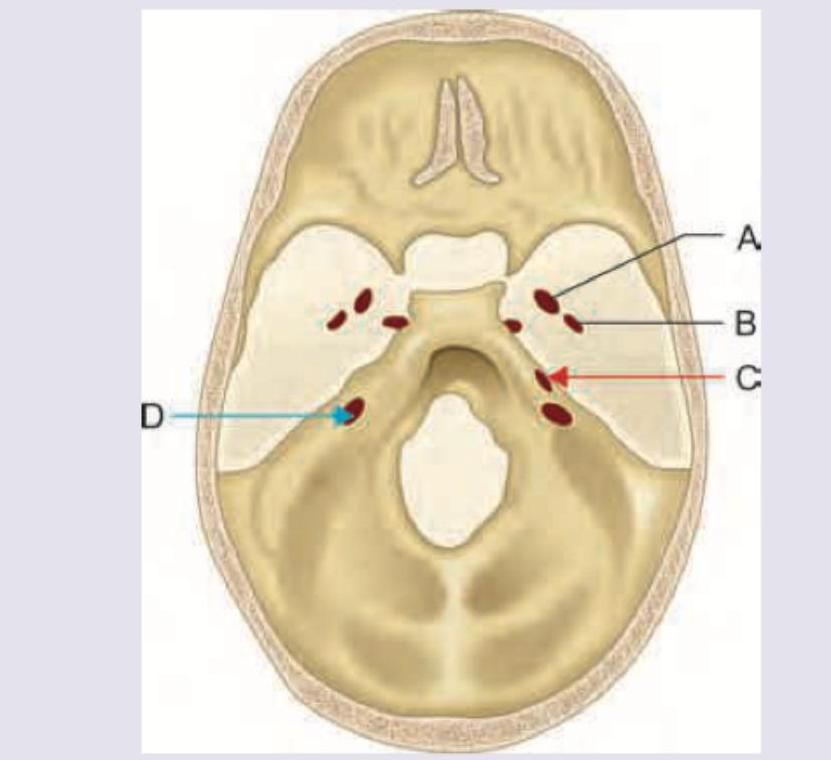
Which nerve passes through the structure shown? (Recent NEET Pattern 2019)

What is the PRIMARY action of the muscle marked in the given image?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app