
Head — MCQs

On this page
Which of the following nerves gives sensory supply to the orbit?
Observe the provided image showing a muscle indicated by an arrow. What is the primary action of this muscle on the mandible?
The image below highlights the jugular foramen. Which of the following does NOT pass through this foramen?
The image below highlights the jugular foramen. Which of the following does NOT pass through this foramen?
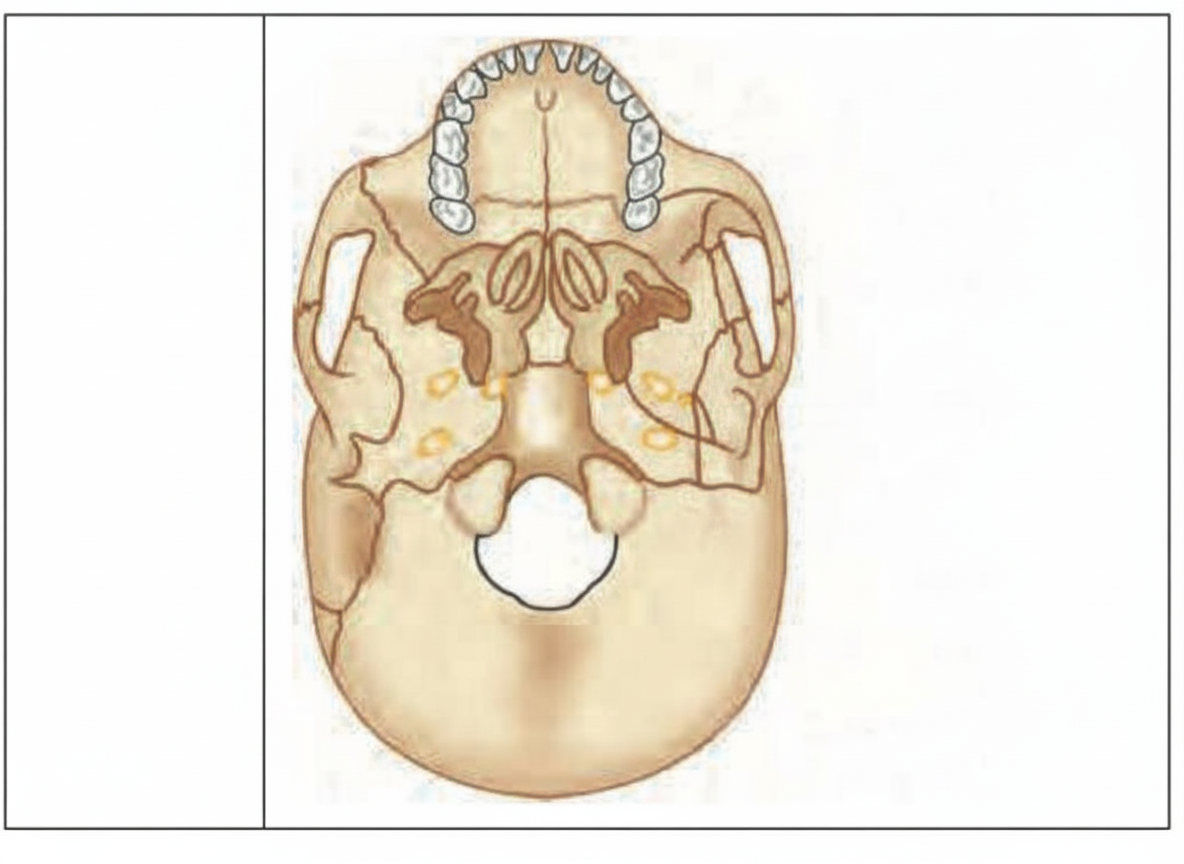
The image below highlights the jugular foramen. Which of the following does NOT pass through this foramen?

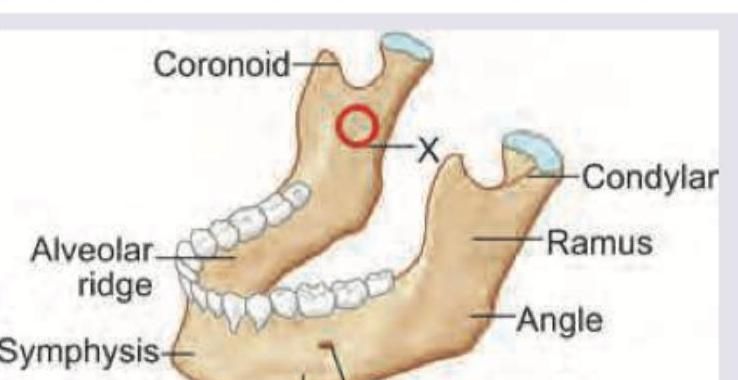
While giving inferior alveolar block, the injection is given above which foramen marked as X ?
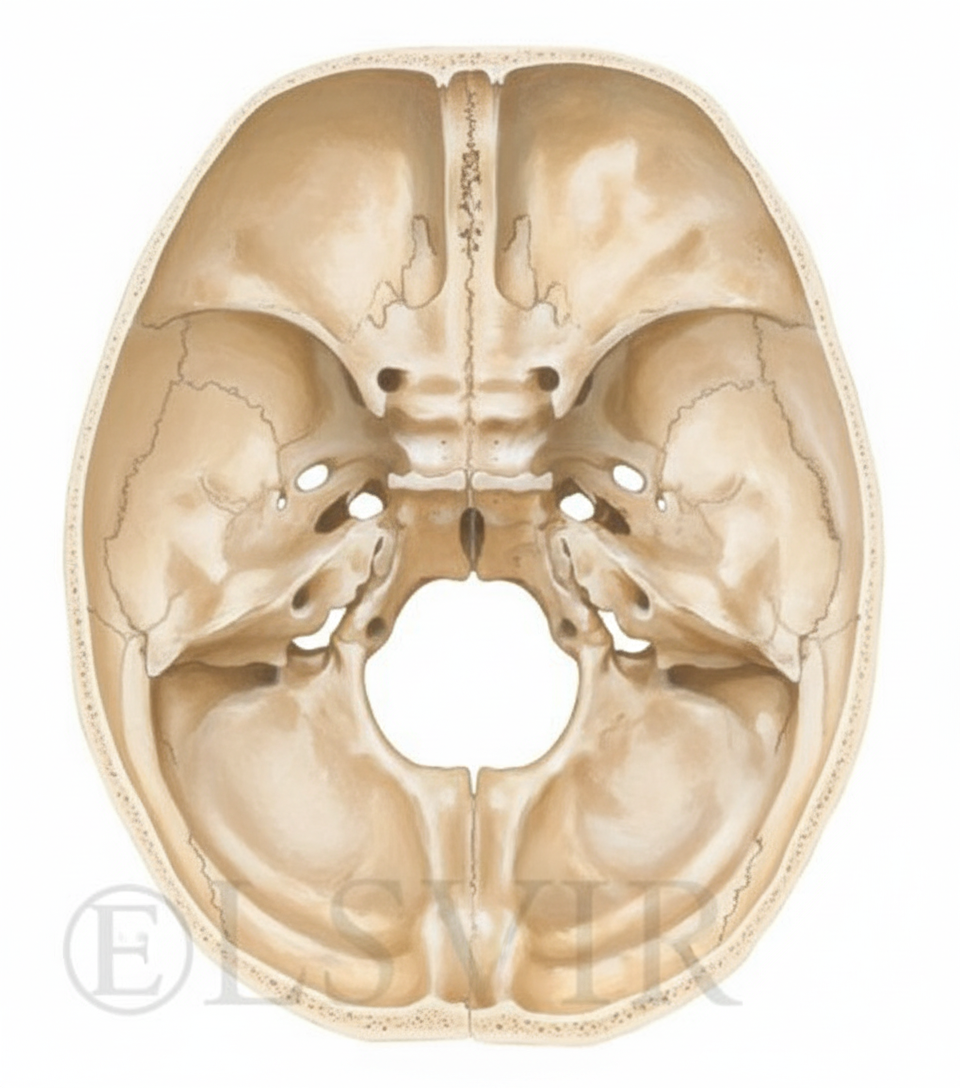
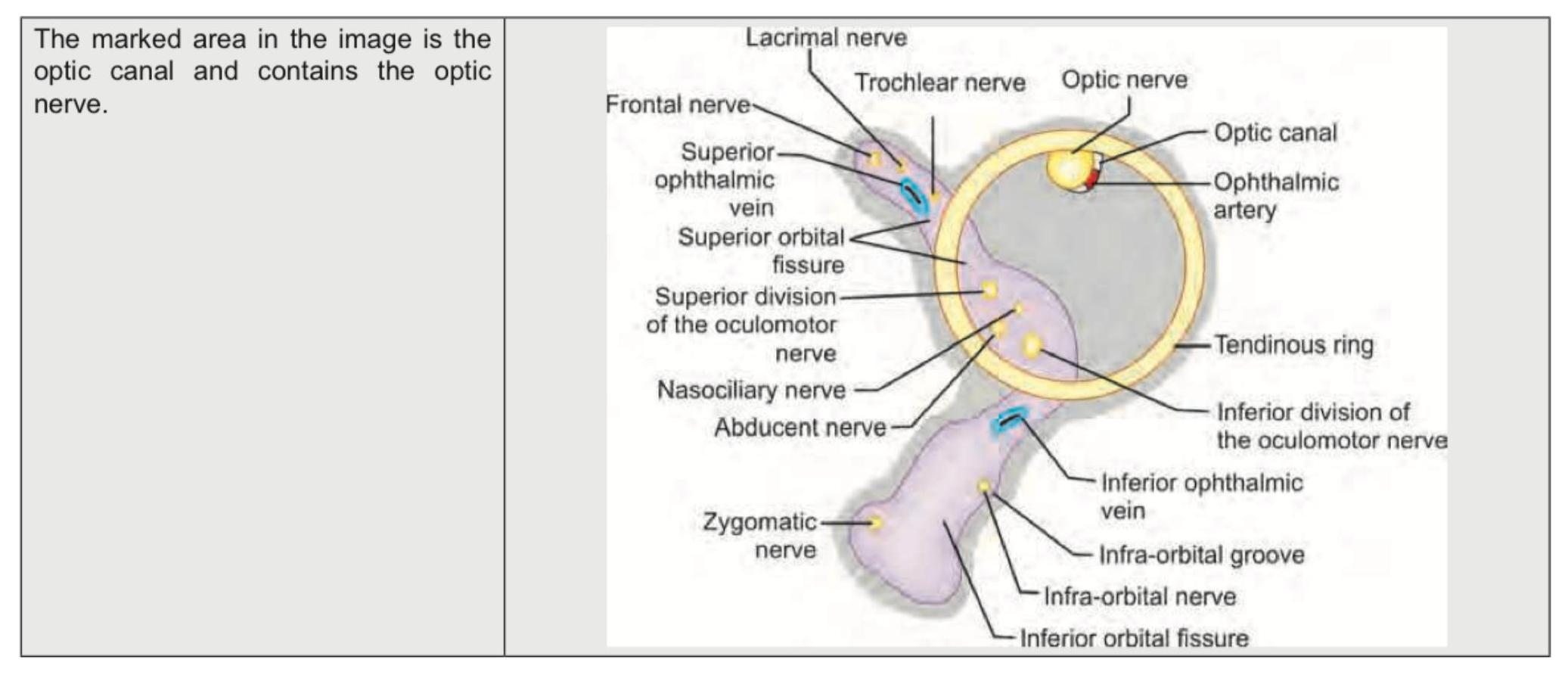
Which of the following foramen transmits the optic nerve?
Which of the following foramen transmits maxillary nerve?
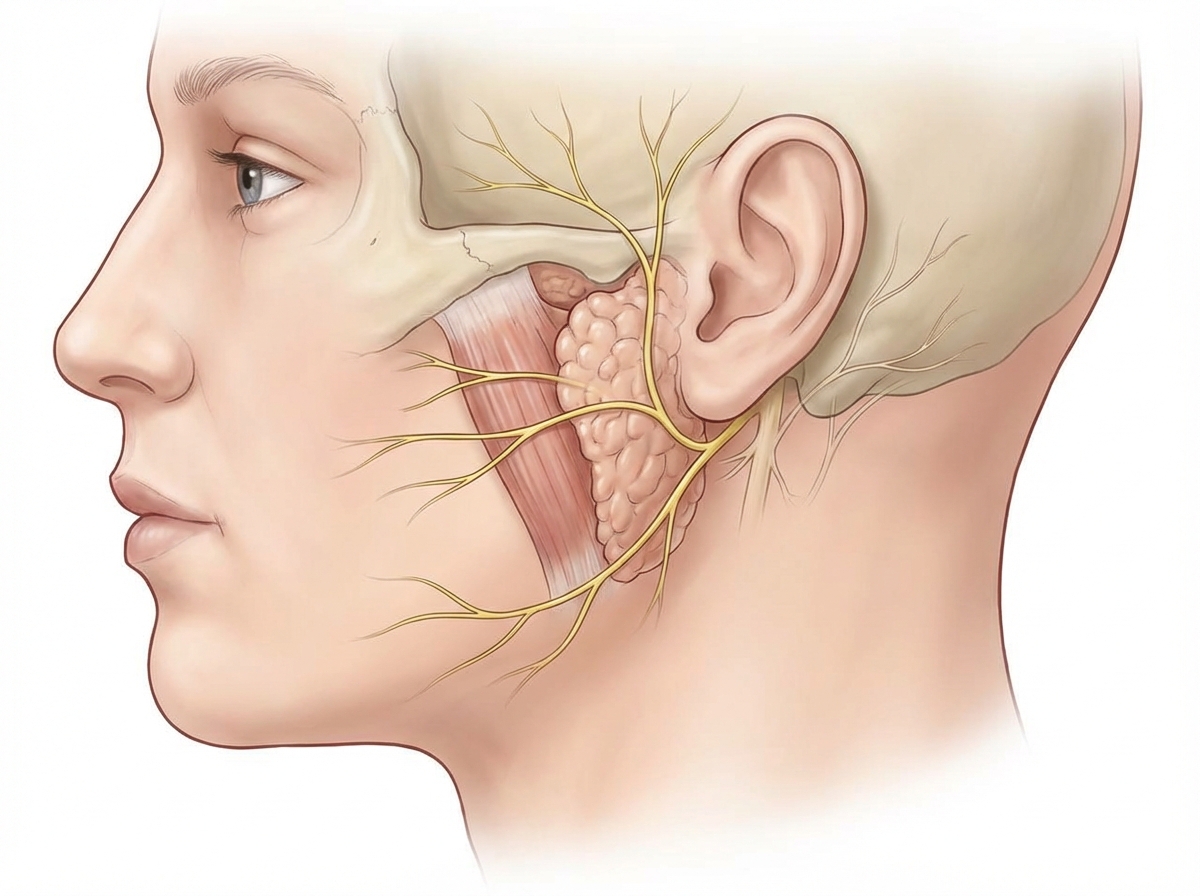
The image shows the parotid gland. Through which ganglion does the secretomotor supply to the parotid gland pass?
80.
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app