
Head — MCQs

On this page
Identify the structure marked in the image given below.
Which nerve innervates the lateral rectus muscle?
Which nerve defect causes lagophthalmos?
In relation to which wall of the orbit are the canaliculi that open into the lacrimal sac present?
Identify the sinus marked in the image.
The framework of the external nose:
Which of the following cranial nerves exits the skull through the jugular foramen?
Identify the part of the occipital bone indicated by the number 3 in the given image.
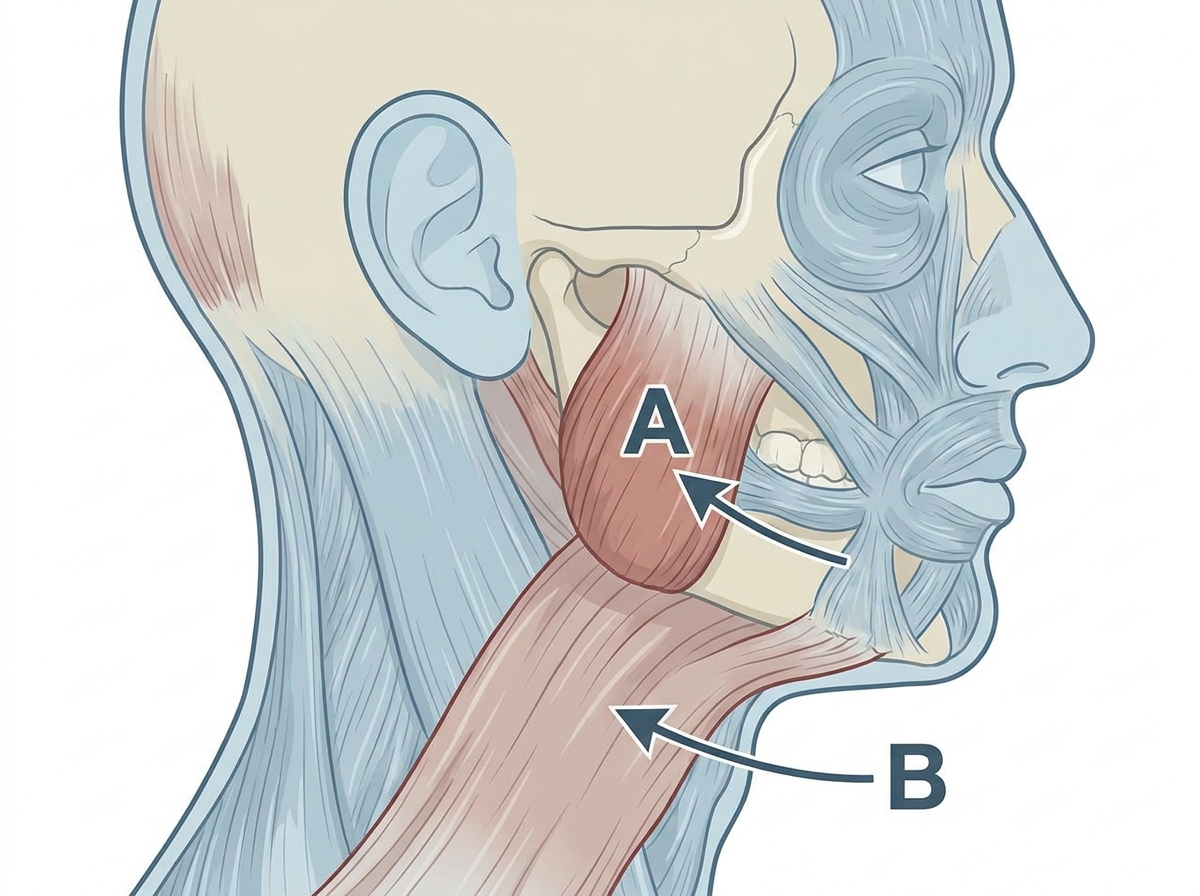
What is the correct nerve supply to the muscles labelled as A and B ?
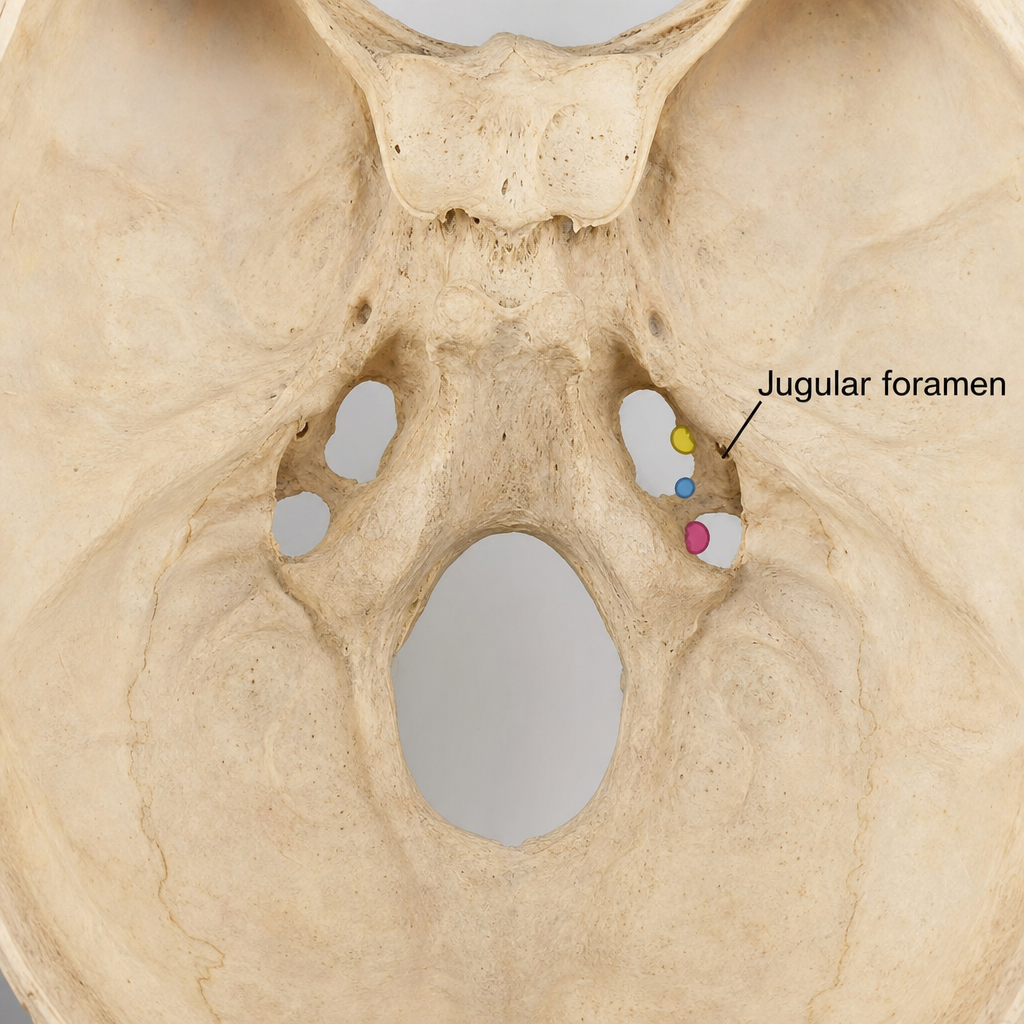
The image below highlights the jugular foramen. Which of the following does NOT pass through this foramen?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app