
Head — MCQs

On this page
What is true about the sphenoid sinus?
Impacted wisdom teeth may produce referred pain via which nerve?
Which nerve supplies the muscles of the tongue?
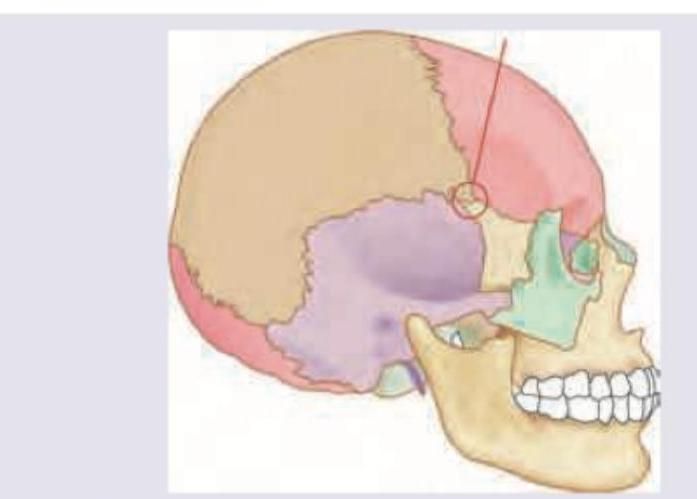
Injury to the marked area of the skull will cause intracranial hemorrhage due to damage to which artery?
The falx cerebri contains all of the following except?
What is the sensory supply of the tongue, excluding which nerve?
Which extraocular muscle facilitates downward rotation, medial rotation, and extorsion of the eyeball?
Which of the following statements about the parotid gland is FALSE?
What is the action of the ciliary muscle?
The Eustachian tube opens into which part of the middle ear cavity?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app