
Head — MCQs

On this page
Which nerve is in close proximity to the internal carotid artery within the cavernous sinus?
Into which part of the nasal cavity does the maxillary sinus open?
A radiograph shows a condition where the total number of teeth present in the oral cavity is one less than normal. What is the most likely diagnosis?
Which of the following cephalic index classifications is characterized by a minimum anteroposterior diameter of the skull relative to its width?
All of the following are true about the middle ear cavity except?
After removal of the parotid gland, a patient experiences sweating on the cheeks while eating. In this complication, the auriculotemporal nerve, which contains parasympathetic secretomotor fibers to the parotid gland, is fused with which nerve?
In a fracture of the optic canal, which pair of structures is most likely to be damaged?
Which of the following muscles of mastication has an opposite and independent function?
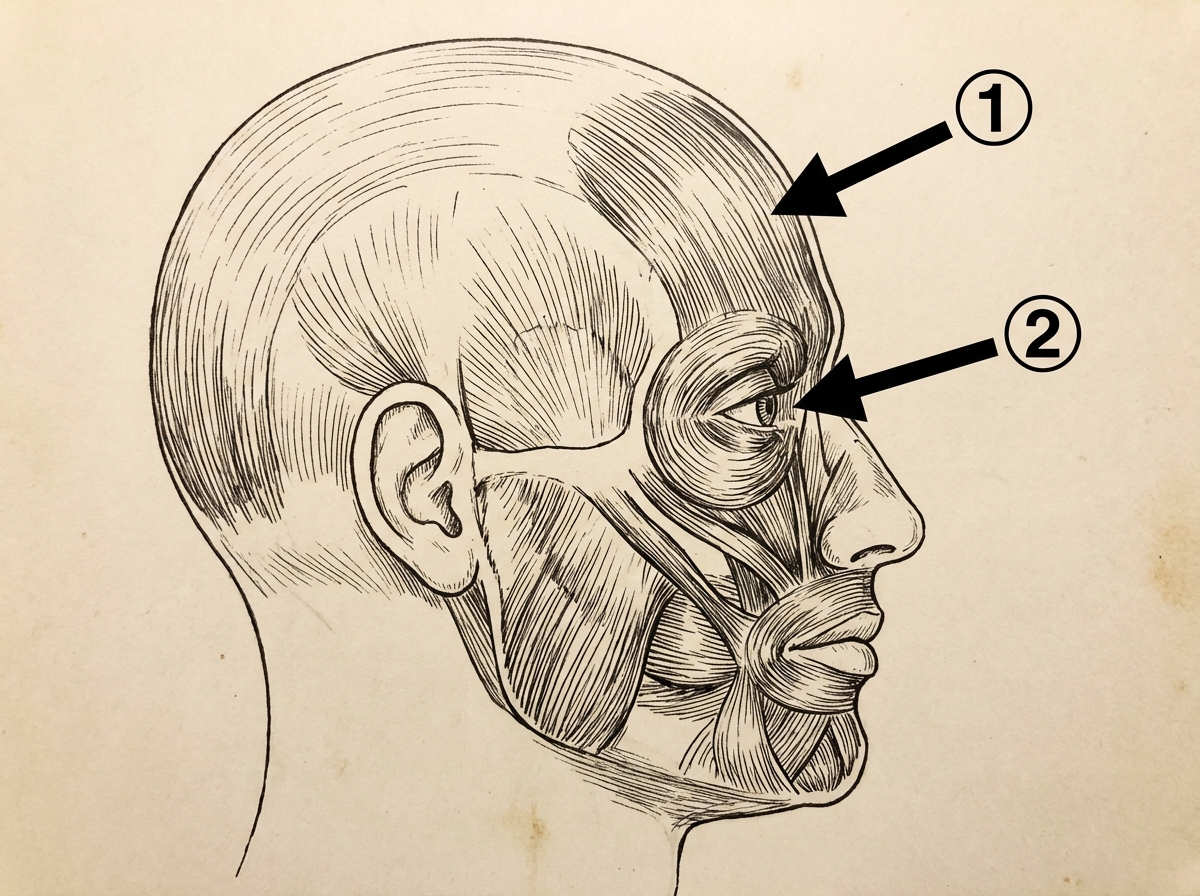
Which nerve supplies the muscle indicated by the second arrow?
What does the Greek letter lambda represent?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app