
Head — MCQs

On this page
Transient Bell's palsy during mandibular nerve block after injection of local anesthesia occurs due to needle piercing into which structure?
The weakest point of the mandible where fracture most commonly occurs is:
Which muscle is the adductor of the eye?
The ophthalmic artery is a branch of which part of the internal carotid artery?
Kiesselbach's plexus is present at which location?
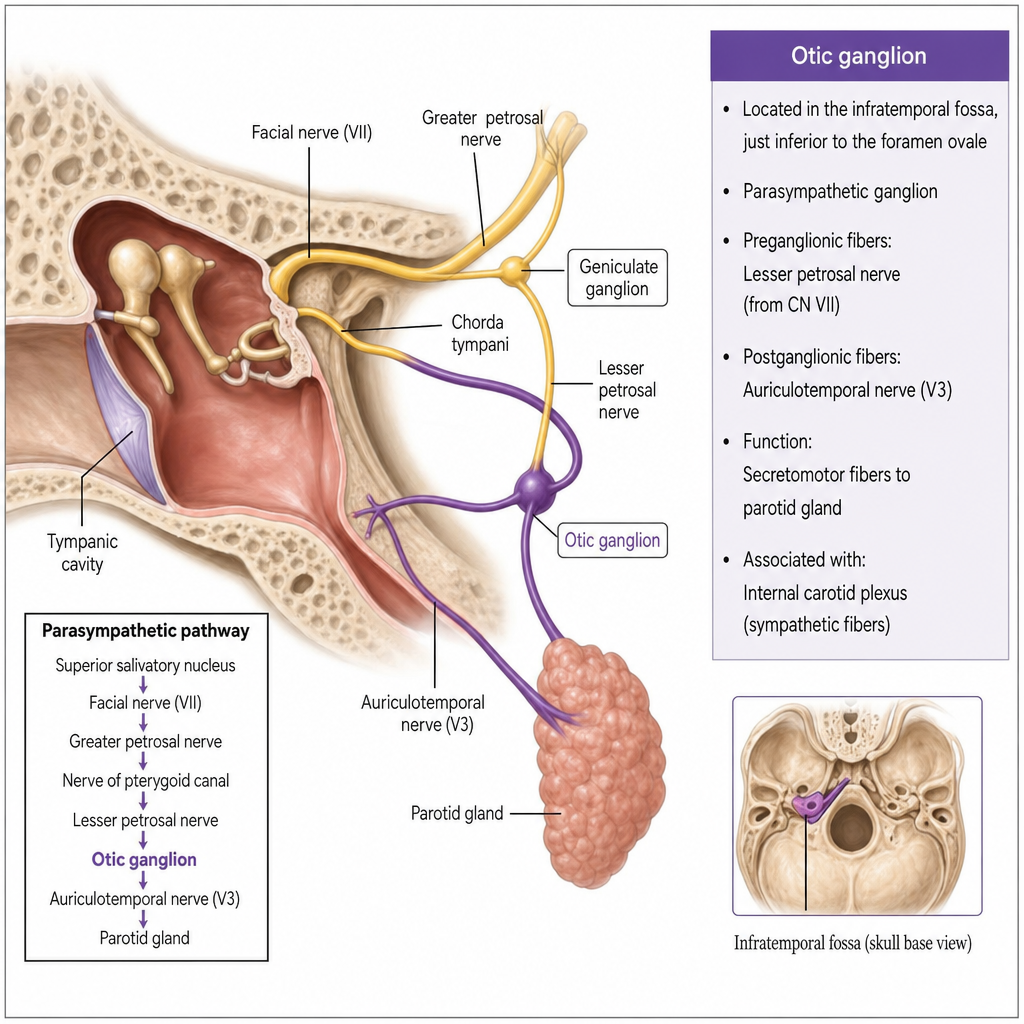
The parasympathetic secretomotor fibres to the parotid gland traverse through which of the following nerves?
Metastases from carcinoma of the tongue by the bloodstream are more likely when the carcinoma involves which of the following parts?
Which of the following statements about the otic ganglion is/are true? 1. It is topographically related to the mandibular nerve (V3) but functionally related to the glossopharyngeal nerve (CN IX). 2. Pre-ganglionic parasympathetic fibers originate in the inferior salivatory nucleus and reach the ganglion via the tympanic plexus and lesser petrosal nerve. 3. Post-ganglionic parasympathetic fibers supply the submandibular gland via the auriculotemporal nerve. 4. Sympathetic fibers pass through the ganglion without synapsing and originate from the plexus around the middle meningeal artery. 5. The motor fibers for tensor veli palatini and tensor tympani that pass through the ganglion are derived from the facial nerve (CN VII).
Injury to which nerve will affect lacrimal secretion?
The nasal septum is formed by all of the following structures except:
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app