
Head — MCQs

On this page
What is the nerve supply of the nose?
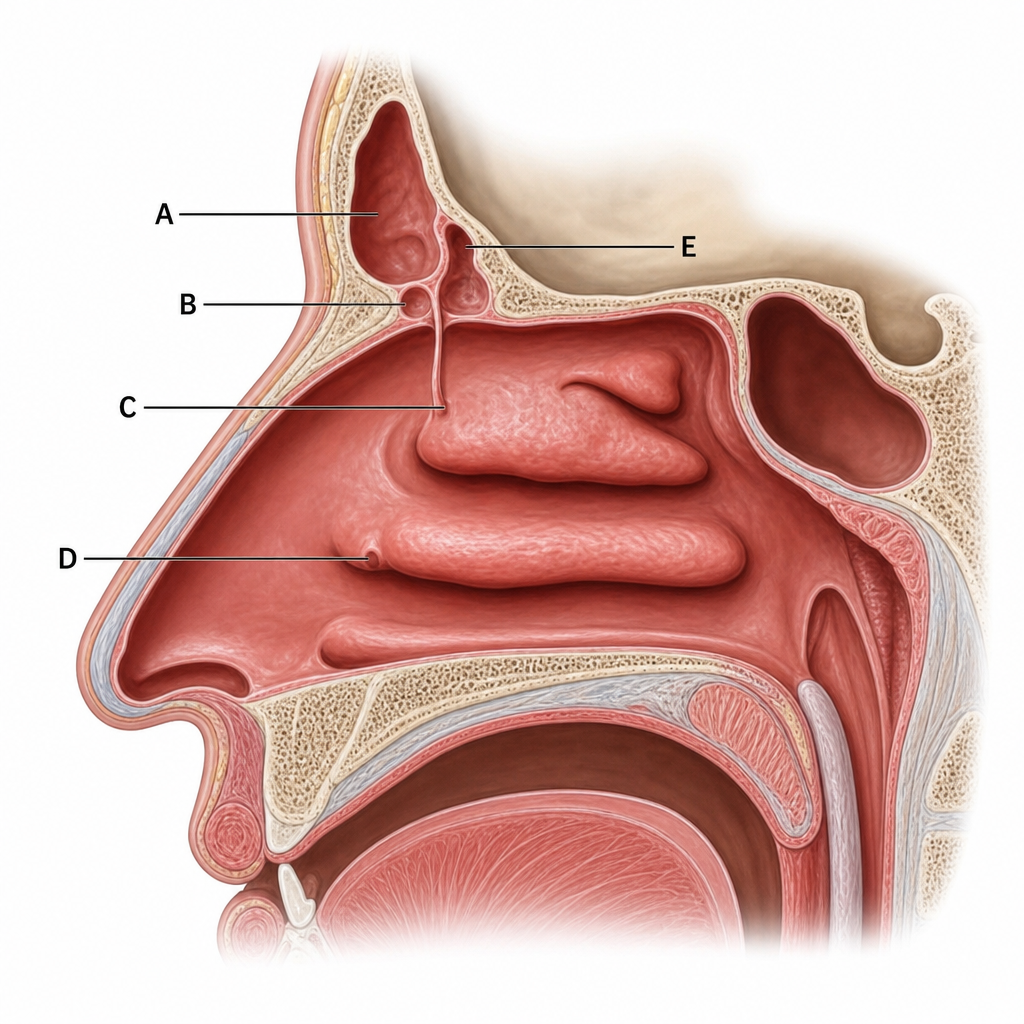
Which structure, when infected, is responsible for spreading infection into the anterior part of the middle nasal meatus through the frontonasal duct?
All of the following are muscles of the nose except?
Chorda tympani is a part of which anatomical structure?
The lateral wall of the nasopharynx shows all of the following structures except?
What is the sensory nerve supply of the middle ear cavity?
What is the arterial supply of the facial nerve?
What is the origin of the maxillary artery?
The anterior part of the scalp drains into which of the following lymph nodes?
A patient presents with the worst headache of their life and sudden, massive epistaxis from the left nostril, which stopped abruptly after nasal packing. There is no history of diabetes, hypertension, local trauma, or surgery. The patient also reports visual loss and unbearable retro-orbital pain. CECT head and DSA were performed. Which extraocular muscle is most likely to be affected in this condition?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app