
Head — MCQs

On this page
Which structure passes through the infraorbital fissure?
In starvation, which component is the last to disappear?
A 35-year-old man presents with severe pain in the right submandibular gland. Radiographic examination reveals a tumor of the gland. During surgical removal of the submandibular gland and its duct, which of the following nerves is most commonly injured?
Frequent dislocation of the temporomandibular joint (TMJ) is most commonly due to which of the following factors?
All of the following supply the temporomandibular joint (TMJ) except?
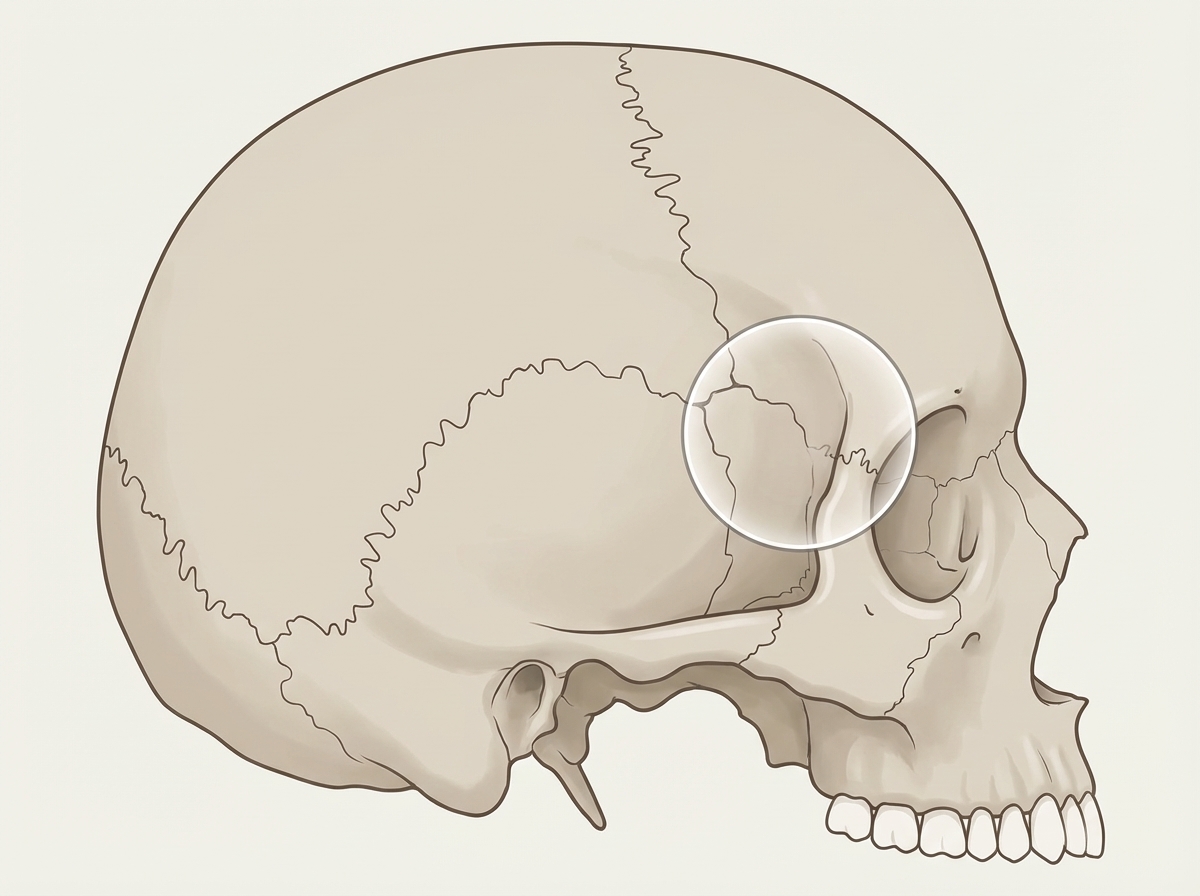
Trauma to the marked area usually results in what type of hemorrhage?
While extracting a maxillary third molar, if one of the roots is found to be missing, the root tip is most likely to be in which space?
What are the cranial nerves that provide parasympathetic nerve supply to the salivary glands?
Which of the following structures attains adult size before birth?
The glands of Moll are modifications of which type of gland?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app