
Head — MCQs

On this page
The nasopharynx extends from which anatomical landmark to which anatomical landmark?
Which of the following cranial nerves travels through the jugular foramen in the base of the skull?
A 36-year-old woman is admitted to the hospital with severe head injuries after a car crash. During neurologic examination, her uvula is deviated to the right. Which nerve is most likely affected to result in this deviation?
What bones form the lateral orbital wall?
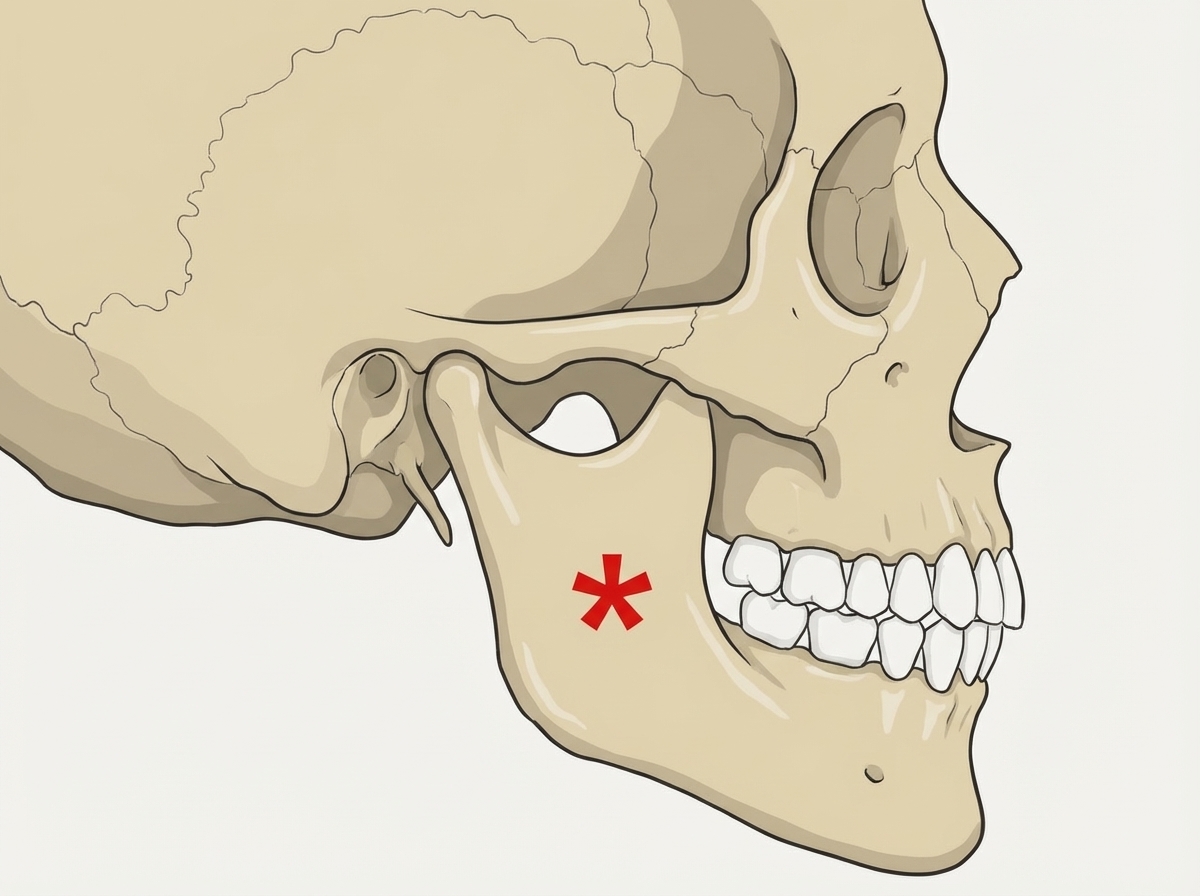
Identify the muscle attached to the marked area in the diagram.
Which extraocular muscle is NOT supplied by the oculomotor nerve?
Which cranial nerve carries pain sensations from the tip of the tongue?
The facial artery terminates in an anastomosis with which of the following?
Which of the following structures does NOT descend through the foramen magnum?
Platycephaly is defined as:
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app