
Head — MCQs

On this page
What is the sensory supply of the parotid gland?
In a case of fracture of the middle cranial fossa, lesion of which of the following structures results in the absence of tears?
The deep part of the submandibular salivary gland is related to which of the following nerves?
What does the arterial ligation of the pterygoid plexus constitute?
A 40-year-old patient presents with dry eyes and reduced nasal secretions. On routine examination, the central nervous system was normal. In which of the following locations might a lesion be present?
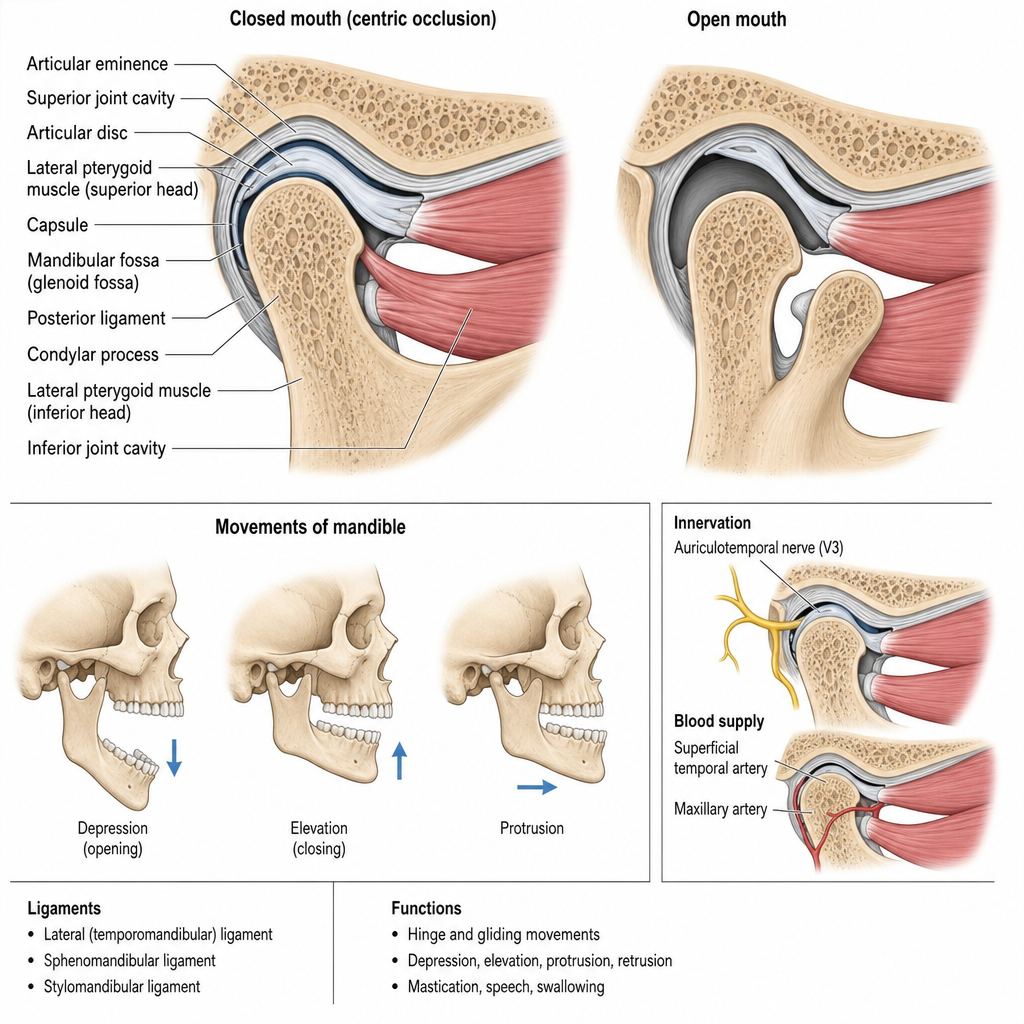
Which of the following statements regarding the temporomandibular joint are true and false? a. The TMJ is a bicondylar synovial joint where the head of the mandible articulates with the mandibular fossa and articular tubercle of the temporal bone. b. The articular surfaces of the TMJ are covered by hyaline cartilage. c. The joint cavity is divided into upper and lower compartments by an intra-articular disc; the upper compartment (meniscotemporal) allows gliding/translational movements such as protrusion and retraction, while the lower compartment (meniscomandibular) facilitates rotatory (hinge) movements. d. The main nerve supply to the TMJ is the auriculotemporal nerve, supplemented by the masseteric nerve.
A patient is asked to protrude their tongue, and salt is placed on the anterior two-thirds of the tongue. This procedure is used for testing which nerve?
Which muscle is primarily responsible for the opening of the jaw?
Which of the following structures is located in the oropharynx?
Which artery is usually torn in a temporal bone fracture?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app