
Head — MCQs

On this page
Which of the following structures does NOT pass through the lateral part of the superior orbital fissure?
Which of the following is NOT a branch of the cavernous part of the internal carotid artery?
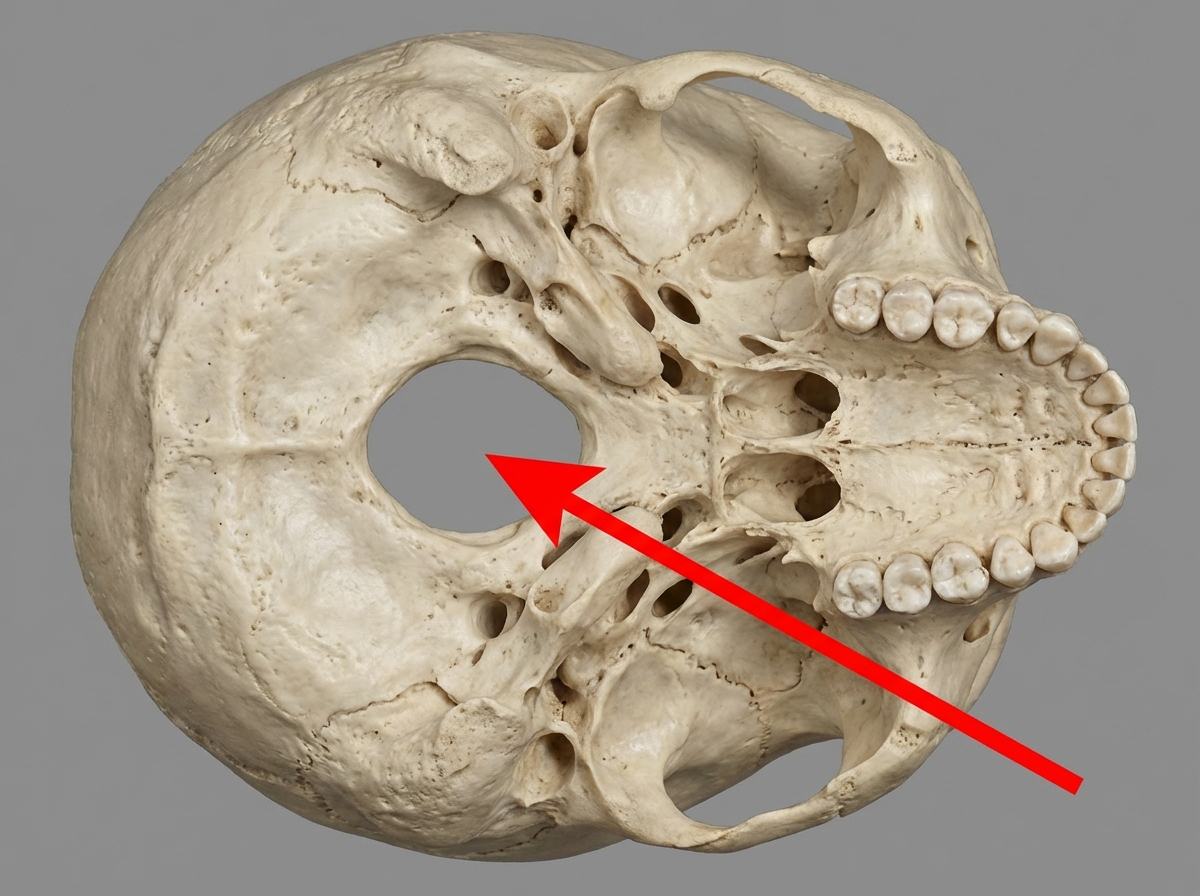
All of the following structures pass through the foramen marked in the diagram EXCEPT?
Which of the following anatomical structures transmits the Internal Carotid Artery?
All of the following are branches of the maxillary artery except?
What is the parasympathetic secretomotor nerve supply to the nose?
A 54-year-old man is admitted to the hospital due to severe headaches. A CT examination reveals an internal carotid artery aneurysm inside the cavernous sinus. Which of the following nerves would be typically affected first?
All of the following structures are present deep to the pterion except?
Which of the following muscles is NOT an abductor of the eye?
Which of the following is NOT a branch of the mandibular nerve?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app