
Head — MCQs

On this page
Which of the following is NOT a muscle of the soft palate?
Ligation of which part of the lingual artery is preferred during surgery for the removal of the tongue in a 40-year-old patient?
A 59-year-old man has difficulty in breathing through his nose. On examination, his physician finds that he has swelling of the mucous membranes of the superior nasal meatus. Which opening of the paranasal sinuses is most likely plugged?
Which statement is NOT true regarding the mandible?
Which muscles are supplied by the facial nerve?
Which sinus connects the cavernous sinus to the transverse sinus?
Which of the following is NOT a content of the middle ear?
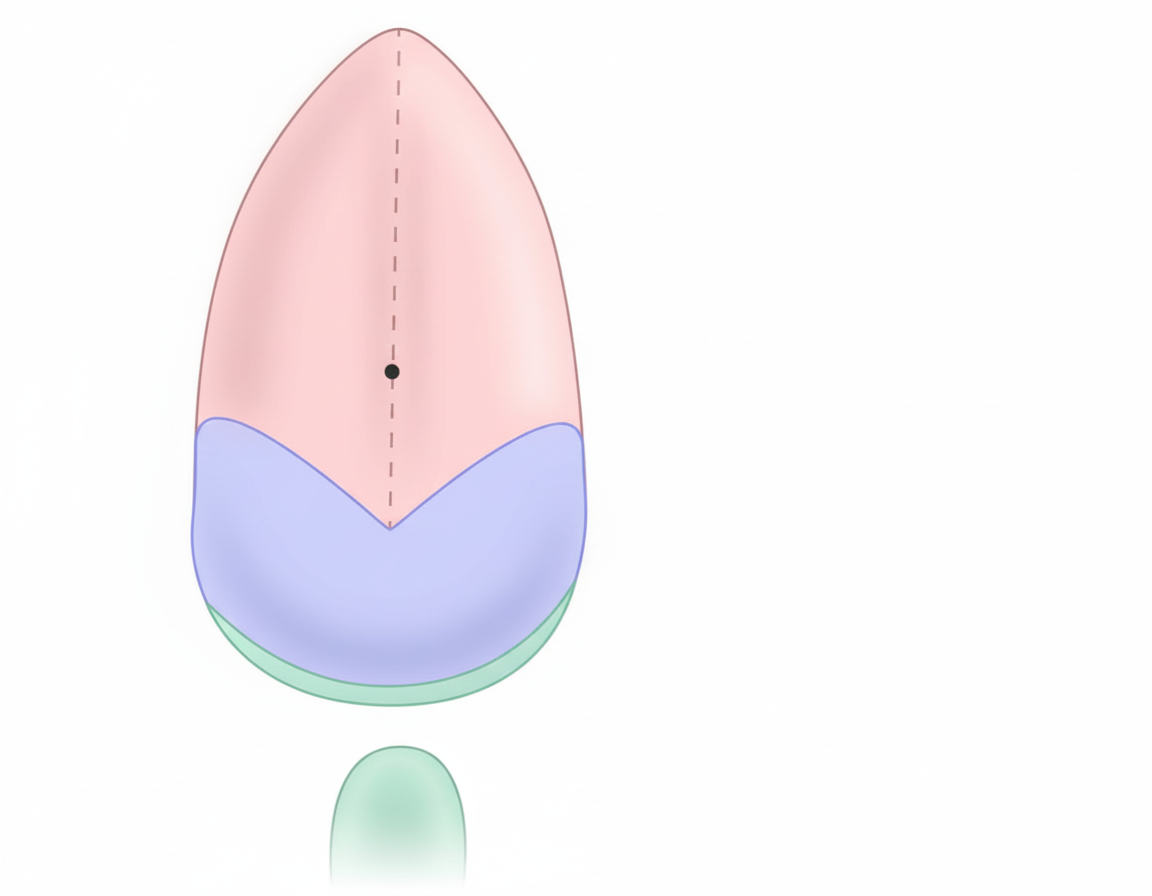
Which cranial-nerve branch supplies taste to the marked area?
Which ganglion supplies secretomotor nerve fibres to the lacrimal gland?
Sympathetic supply to the head is from which of the following spinal cord segments?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app