
Head — MCQs

On this page
Which muscle(s) is/are supplied by the facial nerve?
All muscles of the face are supplied by the facial nerve, except which one?
Which gland is innervated by the pterygopalatine ganglion?
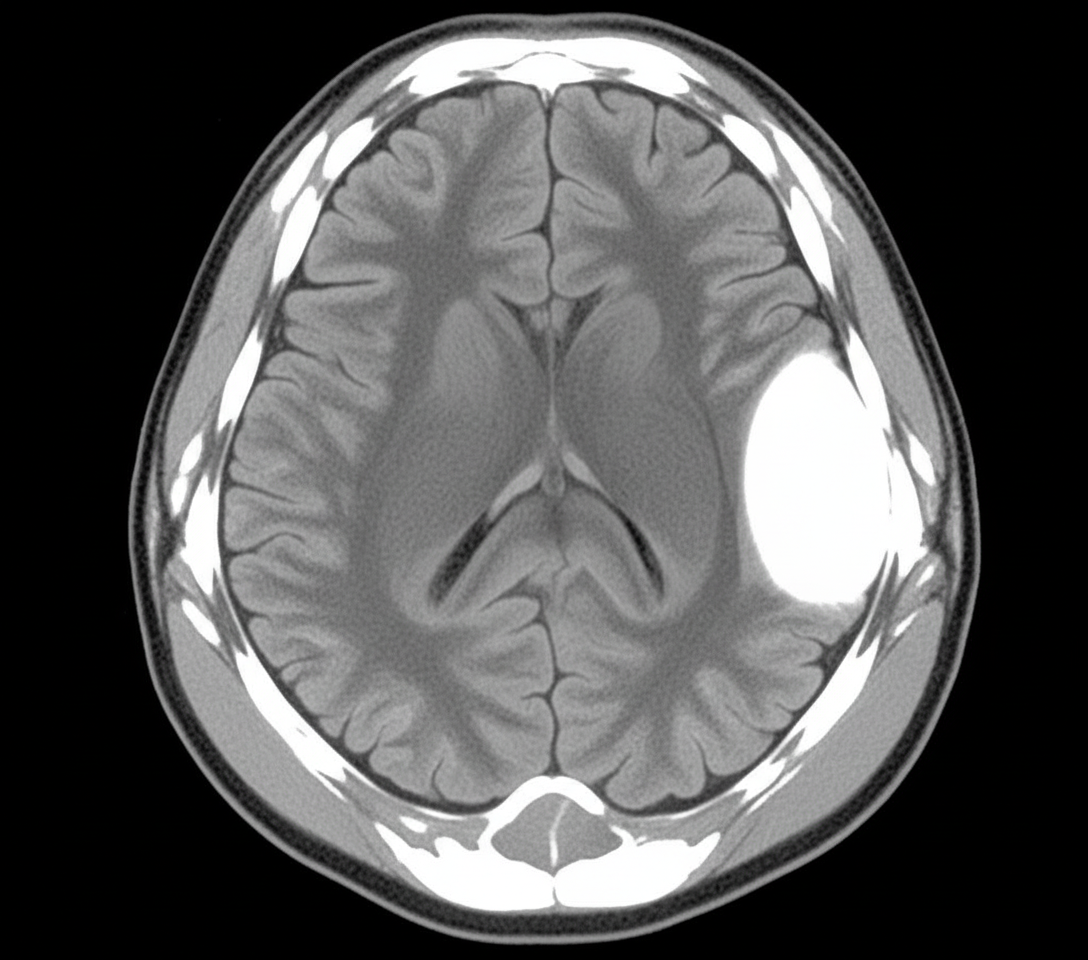
A 20-year-old male presented to the ER with altered sensorium, short-term memory loss, and severe headache after a road traffic accident. There was evidence of skull injury. A non-contrast CT head was performed. The artery most commonly involved in the above condition runs deep to which of the following skull landmarks?
A patient complains of persistent numbness of the chin, lower lip, and lower teeth. She further indicates that she has difficulty chewing. Radiographic studies of the head demonstrated a small discrete mass in the infratemporal fossa. Which nerve has been compromised by the mass?
The palatine bone furnishes the link between which of the following bones?
Into which meatus does the nasolacrimal duct open?
A 26-year-old male sustained a head injury after falling from a ladder. During surgery, the neurosurgeon noticed loss of sensation in the dura of the middle cranial fossa. Which of the following nerves is injured?
Which of the following is NOT a branch of the facial nerve below the stylomastoid foramen?
Horner's syndrome consists of which of the following clinical findings?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app