
Head — MCQs

On this page
Surgical excision of the parotid gland endangers which of the following structures?
What is true about the fovea centralis?
The pterygopalatine ganglion is functionally connected to which of the following nerves?
A 48-year-old male patient complains of diplopia (double vision). On neurologic examination, he is unable to adduct his left eye and lacks a corneal reflex on the left side. Where is the most likely location of the lesion resulting in these symptoms?
Which anatomical structure forms the lateral wall of the middle ear?
Maximum visual acuity in the retina is present on which part?
What is the primary blood supply to the coronoid process of the mandible?
Which nerve hooks around Wharton's duct?
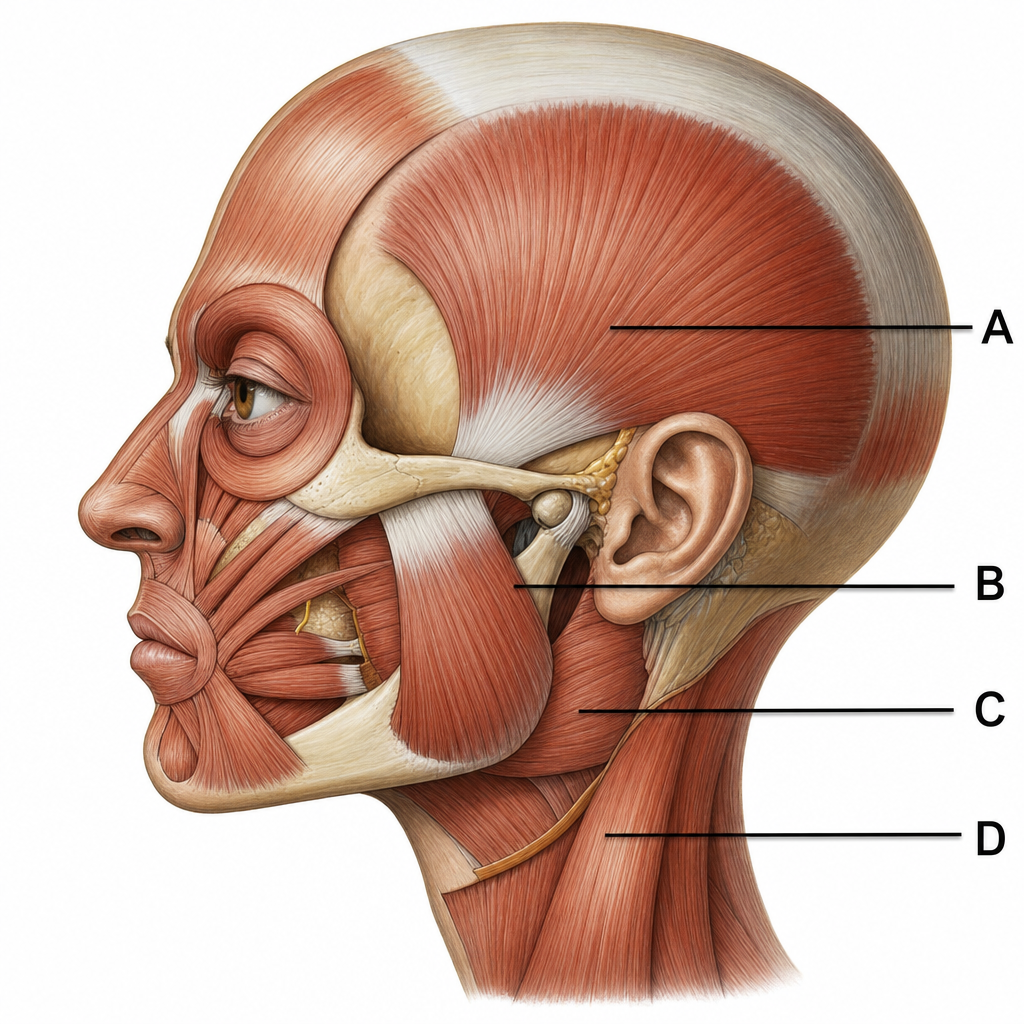
Which of the muscles marked in the diagram helps best to protrude the jaw?
Which of the following carries postganglionic fibers?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app