
Head — MCQs

On this page
Consider the following statements with reference to scalp : 1. The blood vessels lie within dense connective tissue. 2. The anterior scalp is supplied by supraorbital and supratrochlear vessels. 3. The lateral and posterior scalp is supplied by superficial temporal, posterior auricular and occipital arteries. Which of the statements given above are correct?
Important landmark in submandibular gland dissection is:
Which one of the following statements regarding anatomy of fetal head is NOT true?
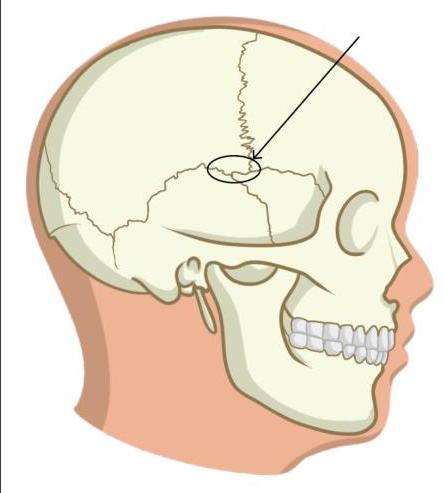
Cephalhematomas are most commonly found over:
A pregnant woman presents with fever, retroorbital pain, headache, pulsatile proptosis of the right eye, and tinnitus. BP and fundus were normal. Which of the following structures are involved?
What is the action of the superior oblique muscle?
Identify the incorrect statement regarding the marked structure.
Masseter is supplied by which nerve?
Cutaneous supply over the parotid gland is by:
Which structure doesn't pass through the parotid gland?
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app