
Head — MCQs

On this page
Paresthesia over the nasal and upper lip following a fractured zygoma is because of involvement of which nerve?
Which of the following structures is included in the posterior segment of the eyeball?
Elevation of the eyebrows and production of transverse wrinkles of the face is characteristic of which muscle contraction?
A 27-year-old woman is admitted to the emergency department after being thrown from a motor scooter. Radiographic evaluation reveals a type I Lefort fracture and comminuted fractures of the mandible and temporomandibular joint. Despite reconstructive surgery, the patient develops hyperacusis due to facial nerve paralysis. Which muscle is most likely paralyzed?
All of the following are structures associated with the pterygopalatine fossa, except:
Which of the following are components of Waldeyer's ring?
A 36-year-old woman is admitted to the hospital with severe head injuries after a car crash. During neurologic examination, it is noted that her uvula is deviated to the right. Which of the following muscles is paralyzed?
Secretomotor innervation to the parotid gland relays in:
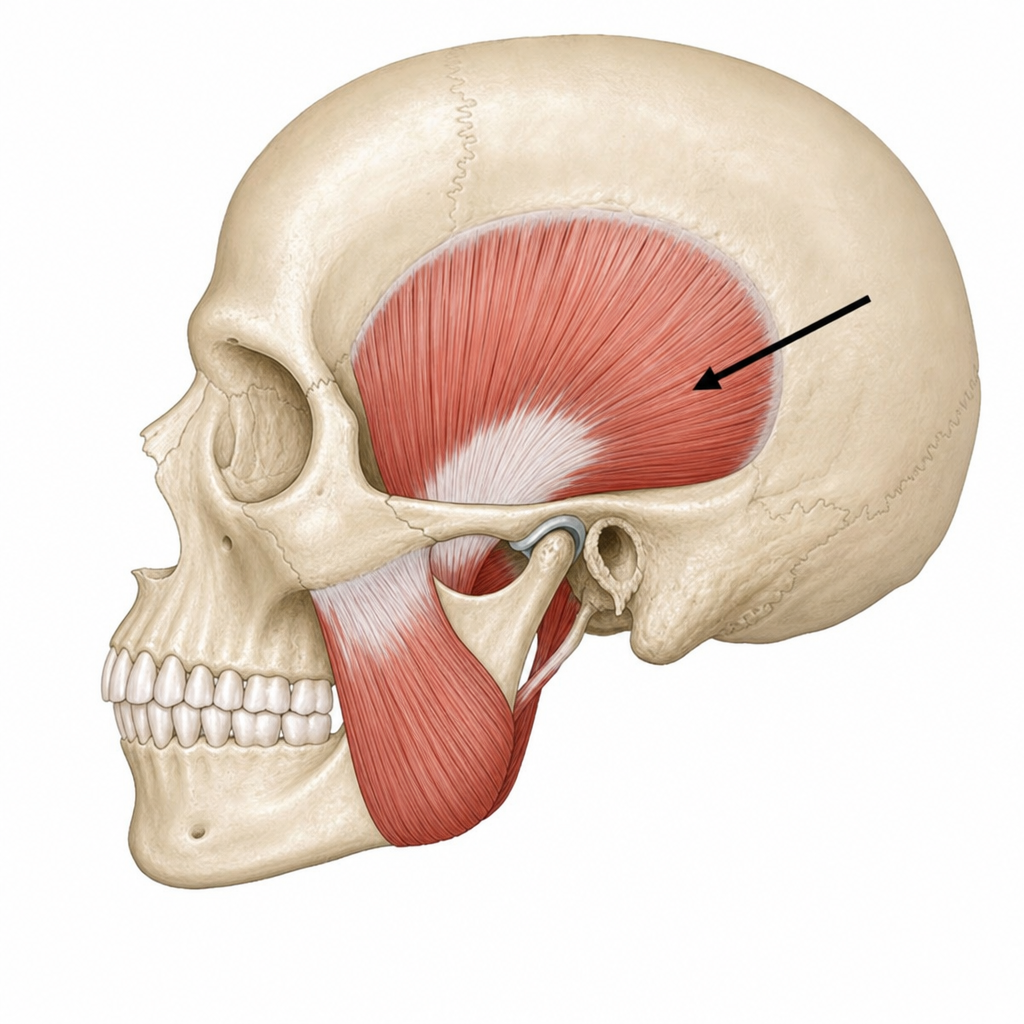
What is the principal action of the posterior fibers of the marked temporalis muscle on the mandible?
All of the following are true of the maxillary artery except:
Practice by Chapter
Skull and Facial Bones
Practice Questions
Scalp and Facial Muscles
Practice Questions
Dural Venous Sinuses
Practice Questions
Cranial Cavity
Practice Questions
Orbit and Contents
Practice Questions
Temporal and Infratemporal Regions
Practice Questions
Pterygopalatine Fossa
Practice Questions
Oral Cavity
Practice Questions
Paranasal Sinuses
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app