
Development of Gastrointestinal System — MCQs

Match the following 1. Hirschsprung's disease 2. Posterior urethral valve 3. Choledochal cyst 4. Intussusception A. Jaundice B. Currant jelly stools C. Distended abdomen D. Oligohydramnios
A 3-month-old with projectile vomiting and olive-shaped mass in abdomen is diagnosed with?
The prostate gland is derived from?
A patient presents with fecal discharge from the umbilicus. What is the most likely diagnosis?
Tenesmus occurs in lesions of the colon.
The labia majora develop from which embryological structure?
Congenital megacolon is confirmed by:
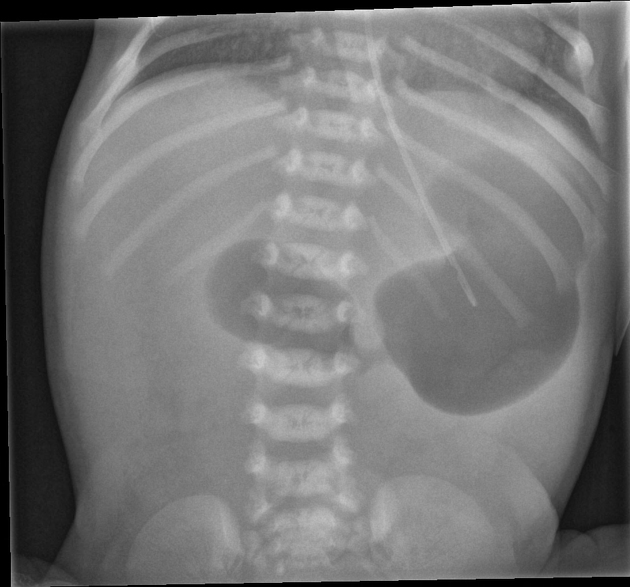
A 6-week-old baby is brought in by the mother with complaints of vomiting. An X-ray shows a single bubble appearance. What is the most likely diagnosis?
Embryologically, from which structure is the cerebellum derived?

The most common site of the branchial cyst is:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app