
Brain and Neuroanatomy — MCQs

On this page
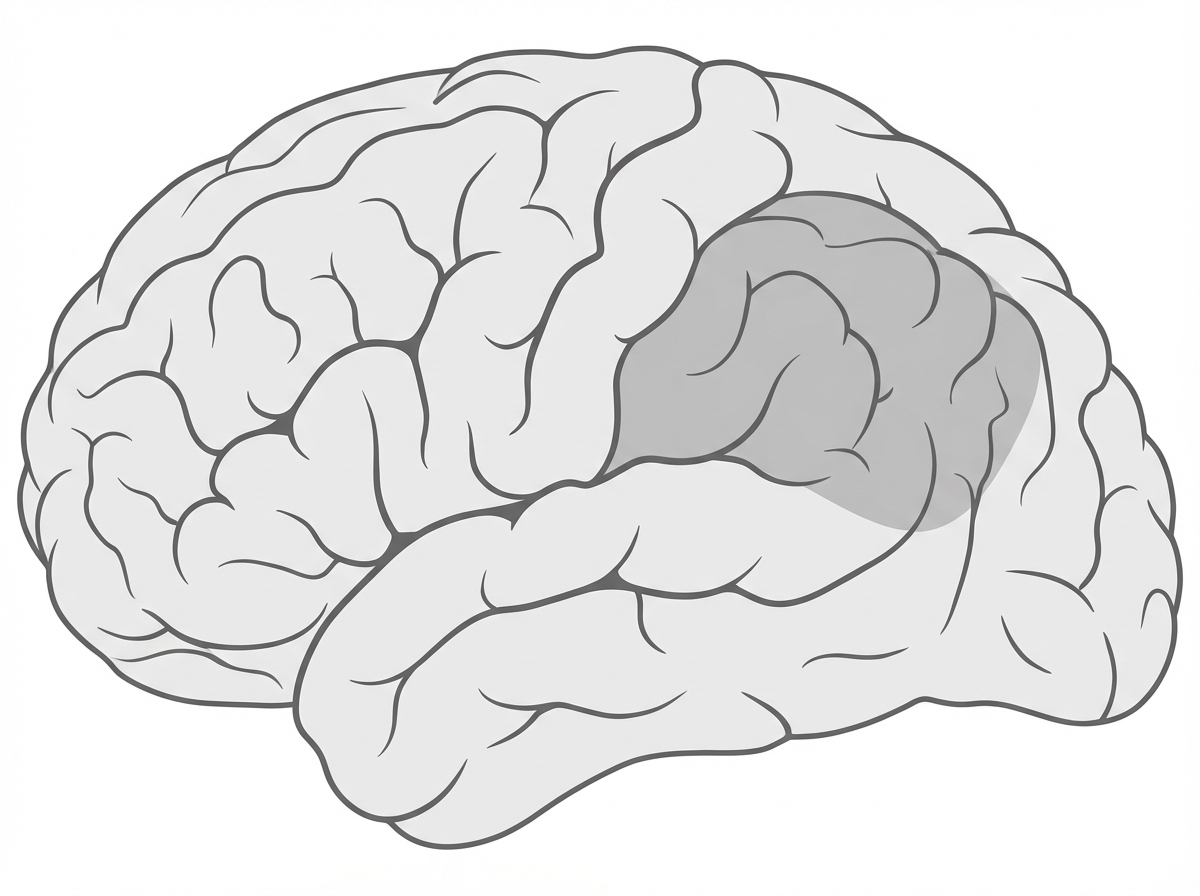
Occlusion of the artery supplying the marked areas will cause which of the following clinical manifestations?
Which of the following is the commonest site for intracranial hemorrhage?
The nucleus of the trigeminal nerve is located in all of the following locations except:
Which part of the internal capsule do the corticospinal fibers pass through?
Which nerve nucleus underlies the facial colliculus?
What is true about the Falx cerebri?
Which is the innermost meningeal layer, that clings tightly to the surface of the brain and spinal cord, following every fold?
Where is the vomiting center located in the brain?
What is the region within the basal ganglia that exhibits the highest density of glutamate receptors?
Which cranial nerves exit the pontomedullary junction?
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app