
Brain and Neuroanatomy — MCQs

On this page
A patient with Parkinson's disease presents with bradykinesia. Which basal ganglia structure is primarily affected?
Which cranial nerve is not directly associated with the eye?
Which nerve is most likely to be injured in a patient with dryness of the mouth following head trauma?
What is the primary role of the corpus callosum?
A patient with a suspected pituitary adenoma shows signs of bitemporal hemianopia. What anatomical feature of the location of the pituitary gland best explains this visual defect?
A 40-year-old woman is being evaluated for severe epilepsy. An MRI shows agenesis of the corpus callosum. What is the function of the corpus callosum?
A patient with a history of melanoma presents with new-onset headache and seizures. An MRI shows multiple brain metastases. Which arterial territory is most commonly involved in brain metastases?
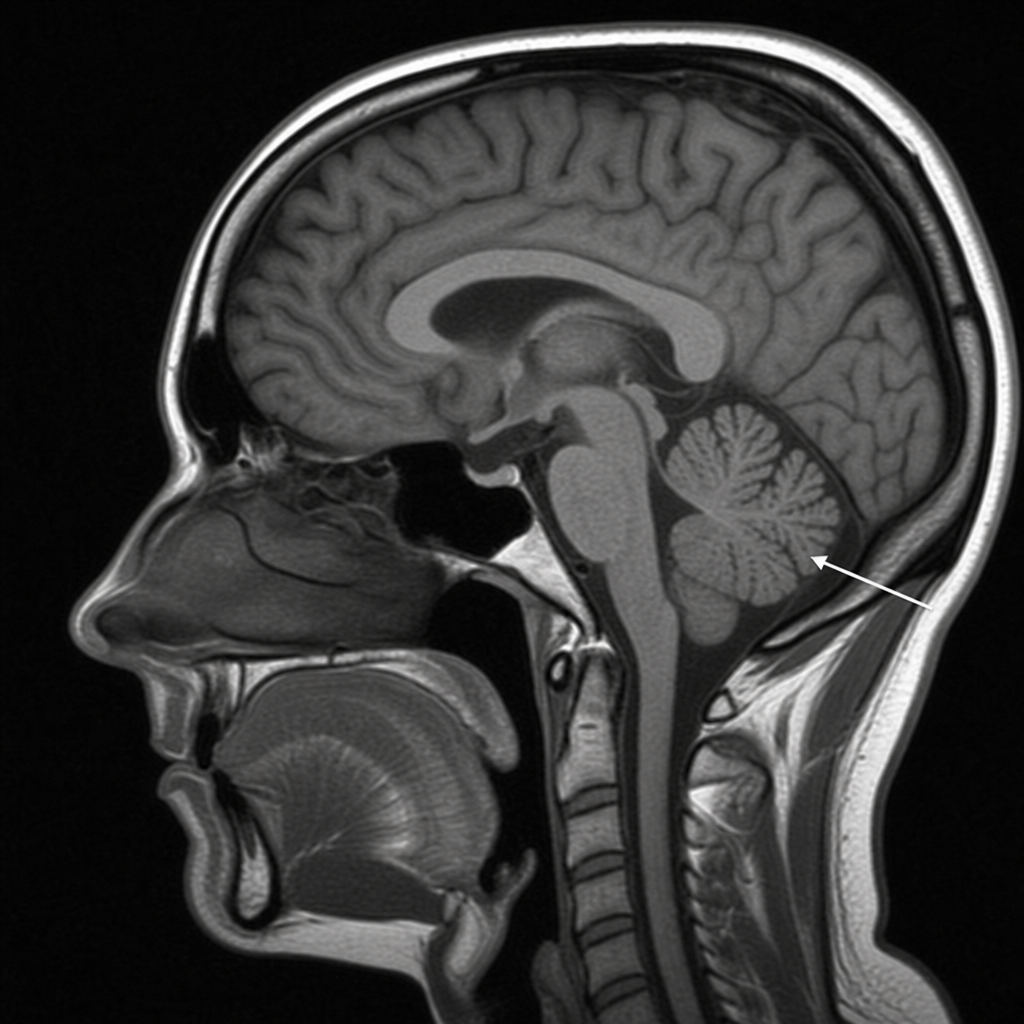
Identify the structure marked in the provided image.
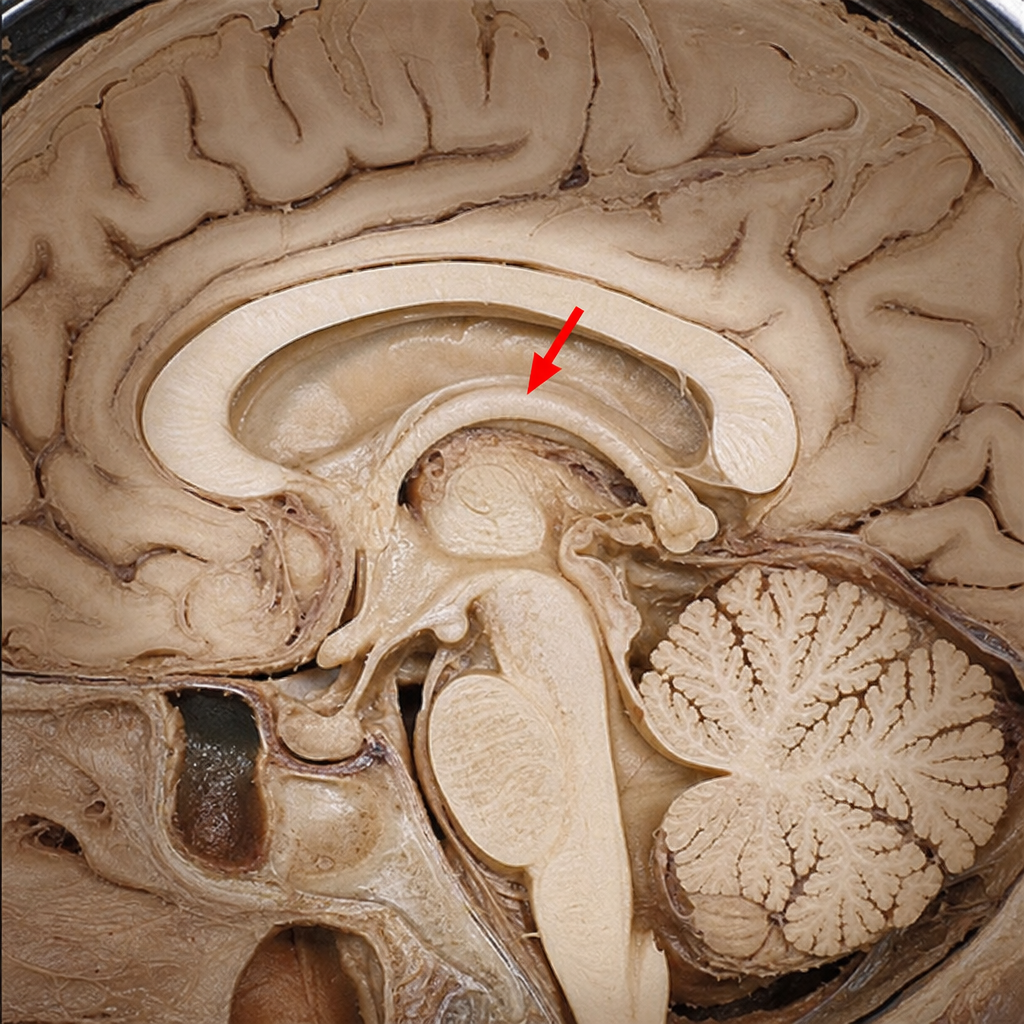
Identify the structure marked by a red arrow in the image provided.
Supramarginal gyrus is a part of?
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app