
Brain and Neuroanatomy — MCQs

On this page
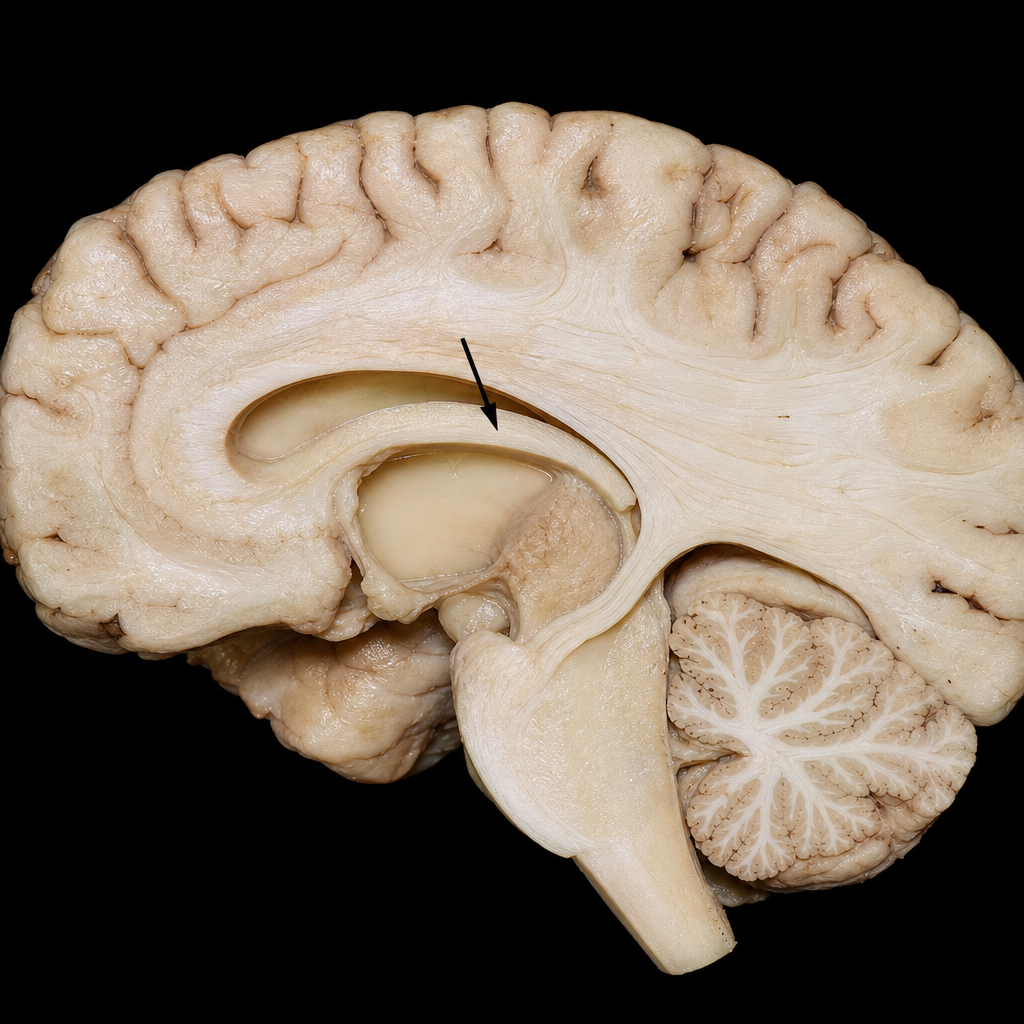
Which of the following projects efferent fibers through the marked structure (fornix)?
A patient presents with sudden onset vision loss and is diagnosed with occlusion of the posterior cerebral artery. Which part of the brain is most affected?
Which lobe of the brain is most involved in auditory processing?
Which structure is NOT present in the floor of the inferior horn of the lateral ventricle?
Spinal sensory nucleus of the trigeminal has 2nd order neurons to carry which sensation?
What does the foramen of Monro connect?
Which artery supplies most of the lateral cerebral cortex?
Which part of the brain is involved in regulating balance and coordination?
Which lobe of the brain is primarily responsible for vision?
A patient with Parkinson's disease presents with bradykinesia. Which basal ganglia structure is primarily affected?
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app