
Brain and Neuroanatomy — MCQs

On this page
A 50-year-old male patient presented with left -sided hemiparesis. Damage to which part of the internal capsule leads to this presentation?
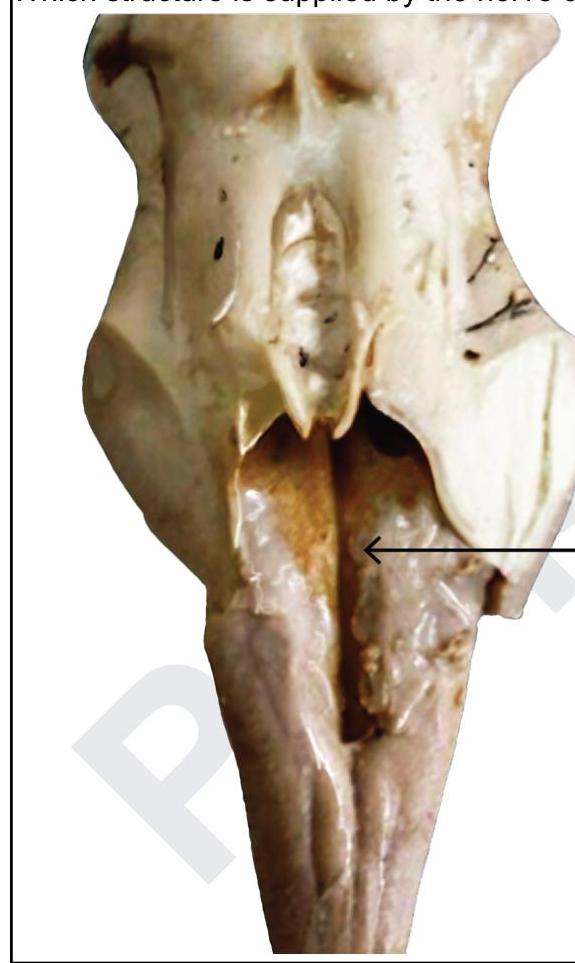
Which structure is supplied by the nerve causing this elevation?
What is the correct sequence of the auditory pathway?
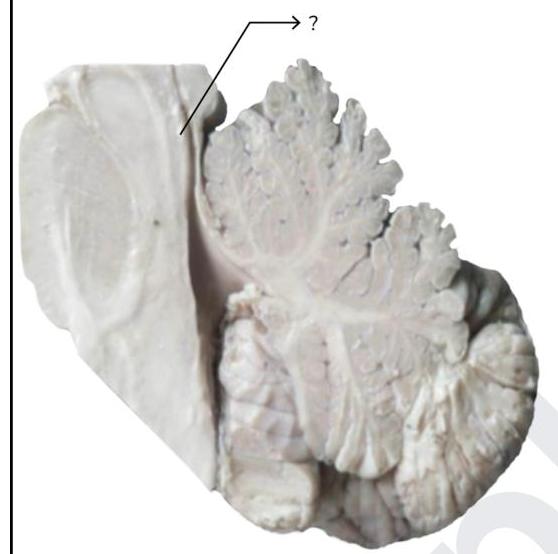
Fibers from the marked structure terminate at which of the following?
Which structure connects Broca's area and Wernicke's area?
Visual loss due to cerebral degeneration is related to which artery?
Most medial nucleus of cerebellum is:
Which of the following nerves transmits impulses originating from the vestibular apparatus?
Mark the false statement regarding nucleus of facial nerve :
Visual processing center is located in -
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app