
Brain and Neuroanatomy — MCQs

On this page
Which structure is marked with a red arrow in the image shown below? (AIIMS May 2018)
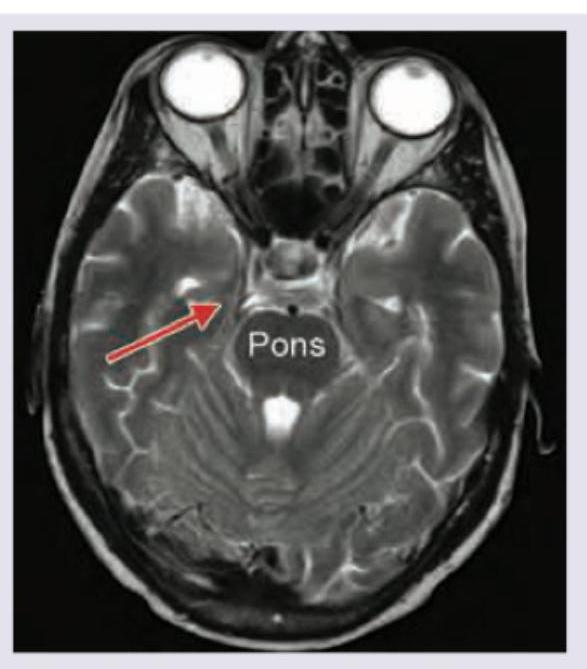
The marked extraocular muscle has a cranial nerve nucleus. At what level in the brain is the nucleus located? (AIIMS May 2018)

Which disease occurs due to involvement of the structure marked in red? (AIIMS May 2018)
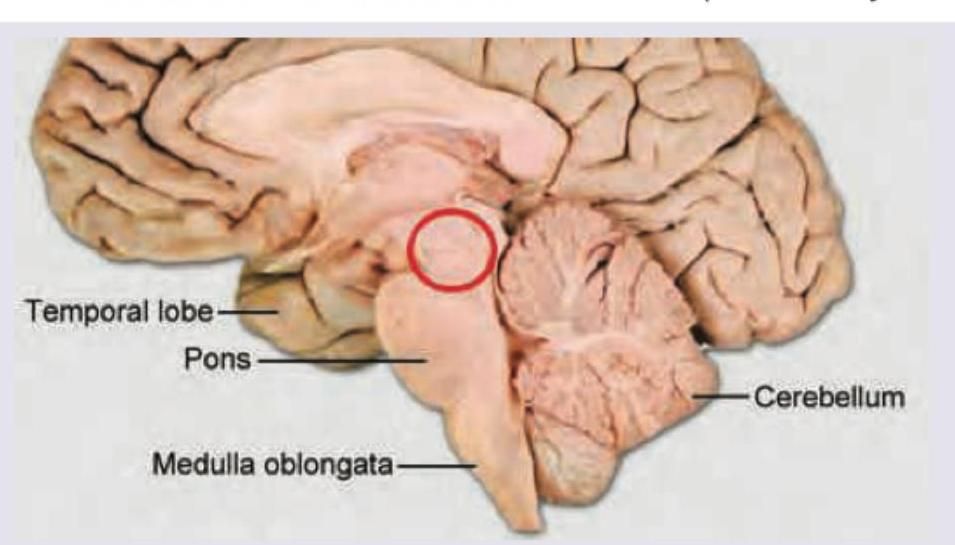
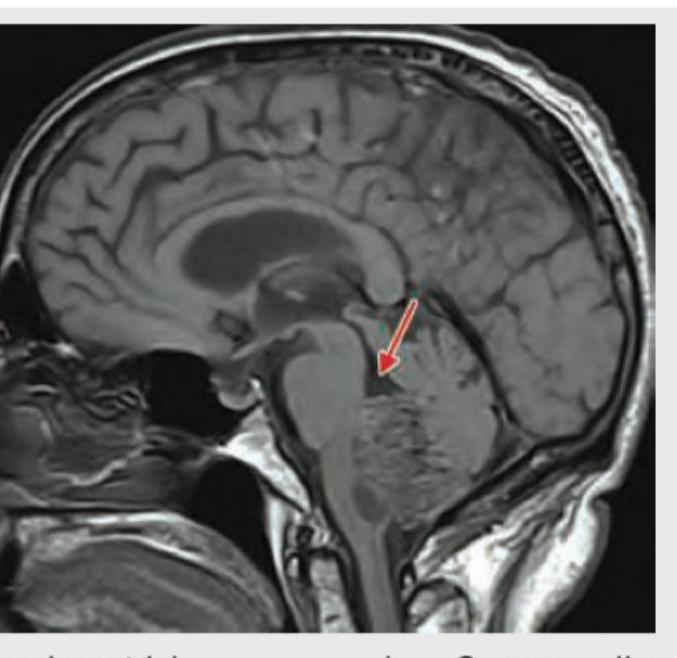
Identify the structure shown. (Recent NEET Pattern 2019)
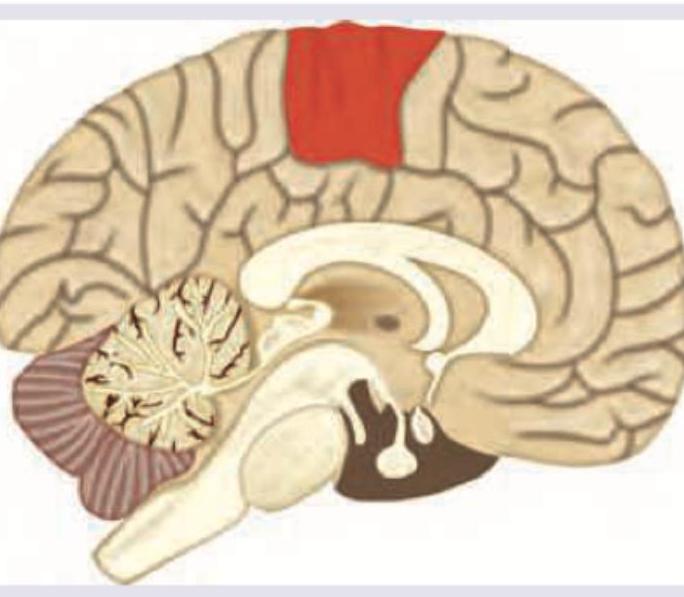
Bilateral occlusion of the anterior cerebral artery (ACA) supplying the area marked in red (paracentral lobule and medial cortex) will lead to all of the following except:
What is the name of the marked blood vessel in the Circle of Willis?
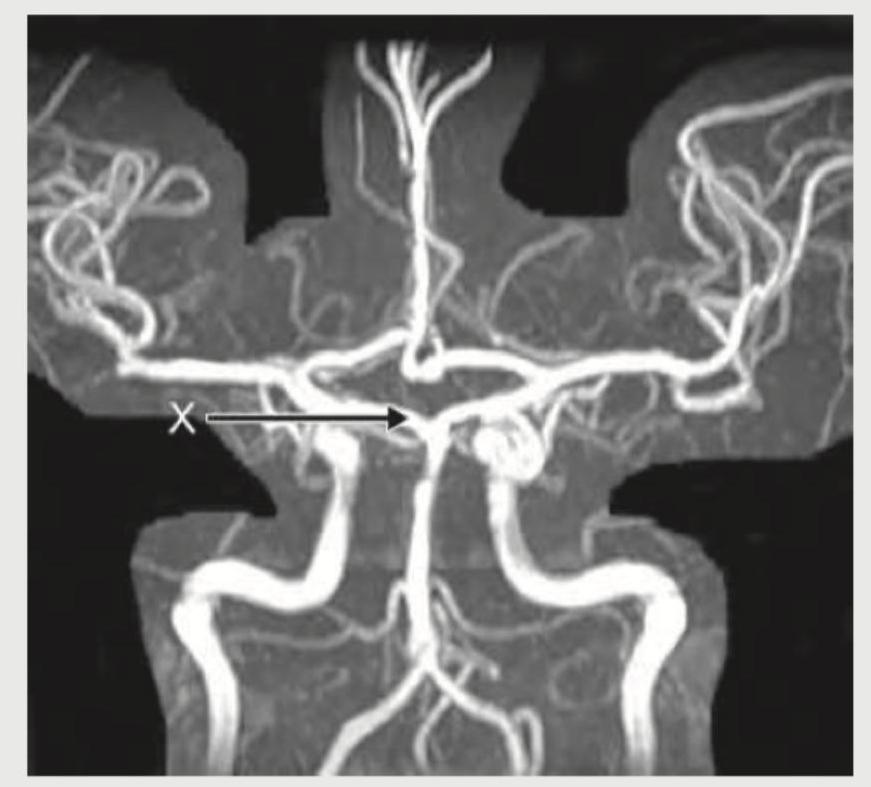
What is the name of the marked blood vessel shown in brain circulation?

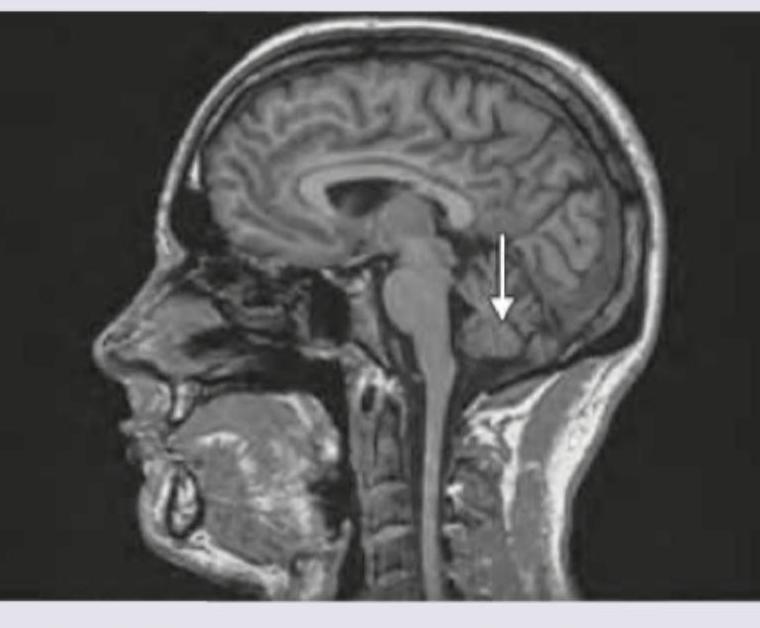
Identify the image given below.
The glymphatic system is the lymphatic-like structure of which system?
Contralateral Homonymous upper quadrantanopia is the type of visual loss seen when the lesion is located at which one of the following anatomical locations?
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app