
Brain and Neuroanatomy — MCQs

On this page
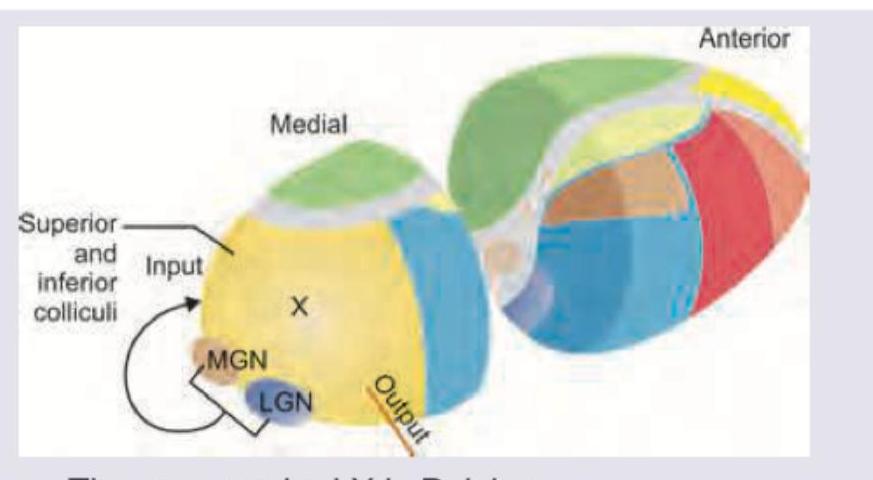
This part of thalamus is linked to medial and lateral geniculate body. Identify the incorrect statement about the area marked as $X$.
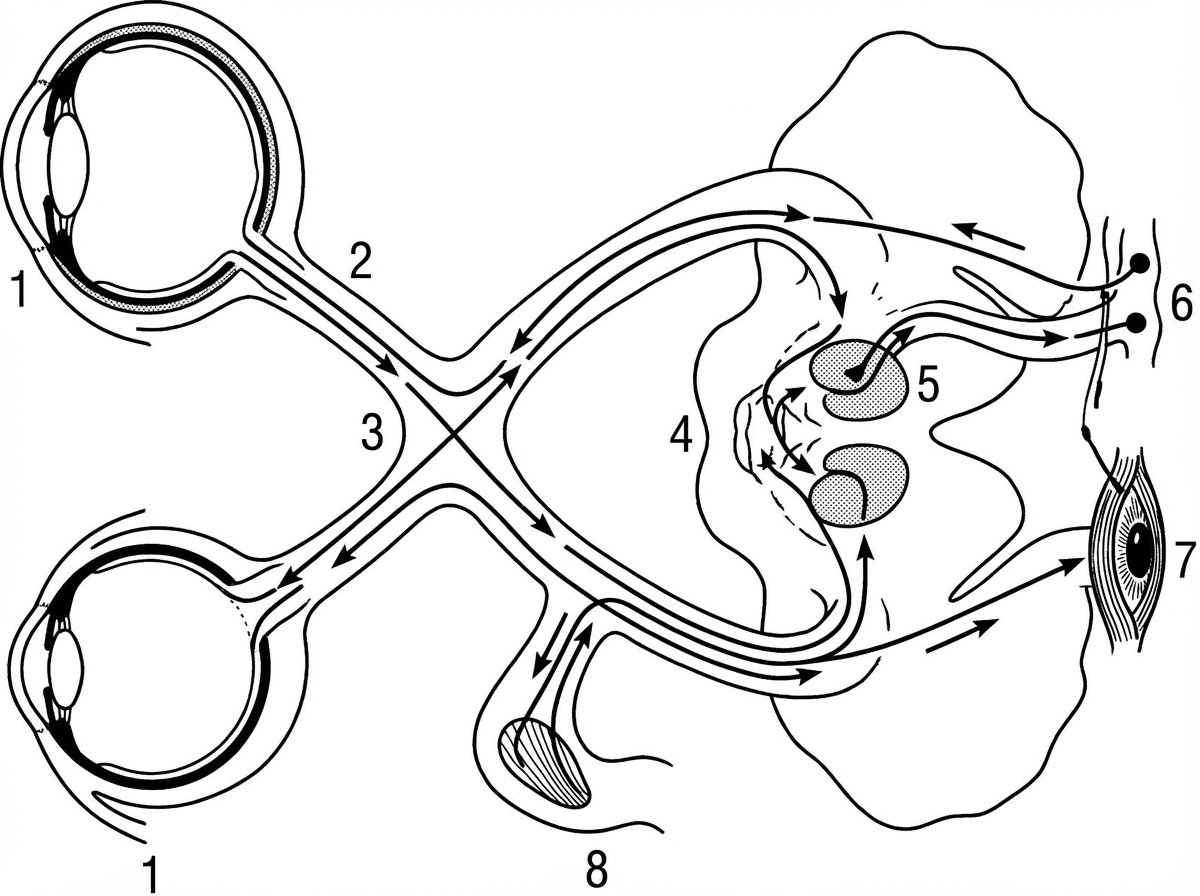
The pathway of light reflex is shown. Lesion of which of the following areas results in development of Argyll Robertson pupil?
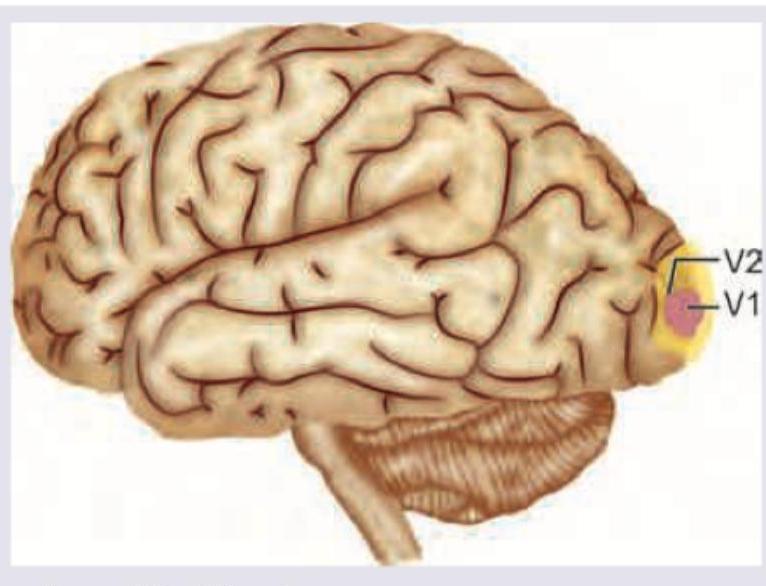
All are true about the area shown except:
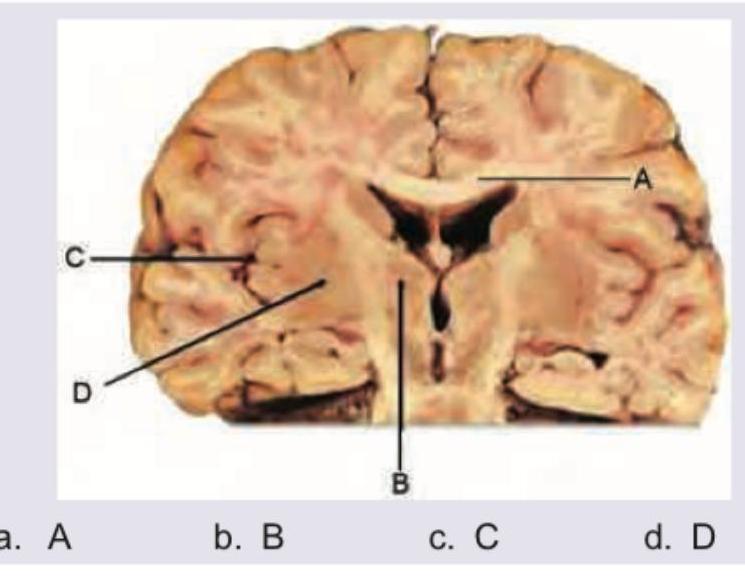
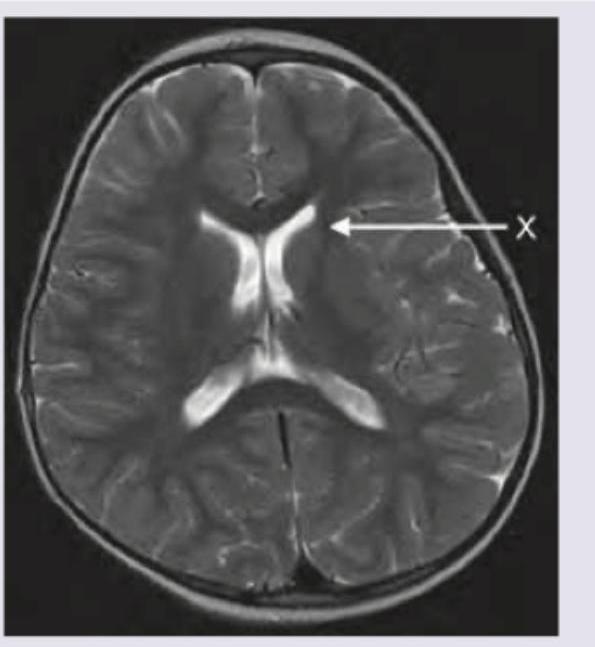
Which of the following depicts insula in the cross section of the brain?
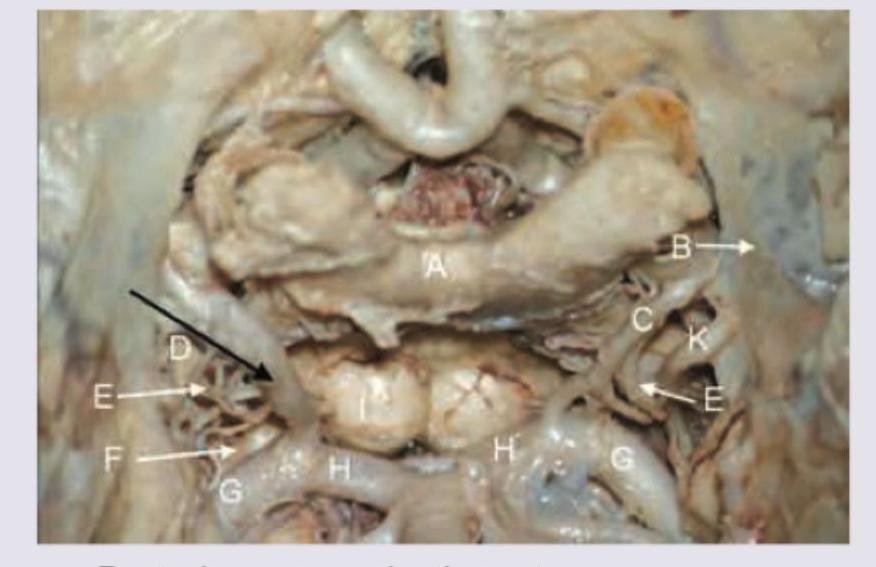
Identify the artery labelled with black arrow in the given diagram.
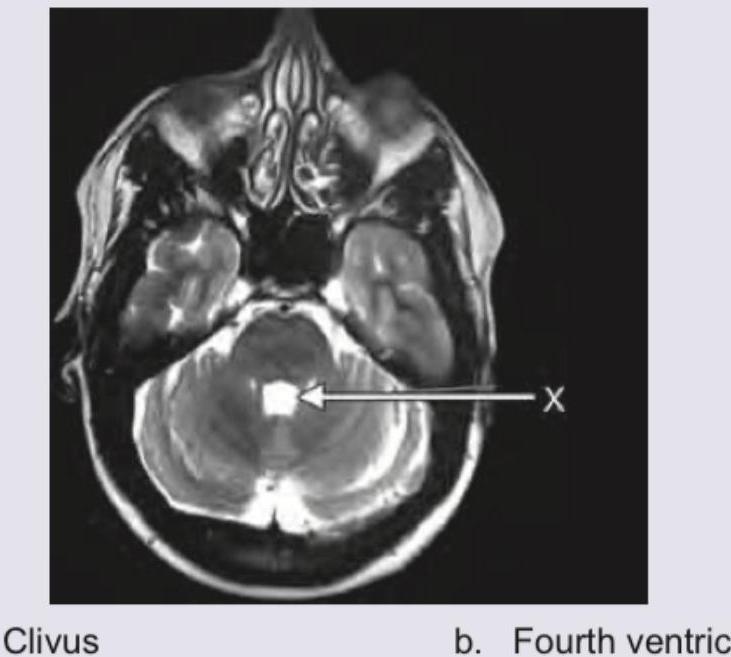
The structure marked as $X$ is:
The structure marked by arrow is:
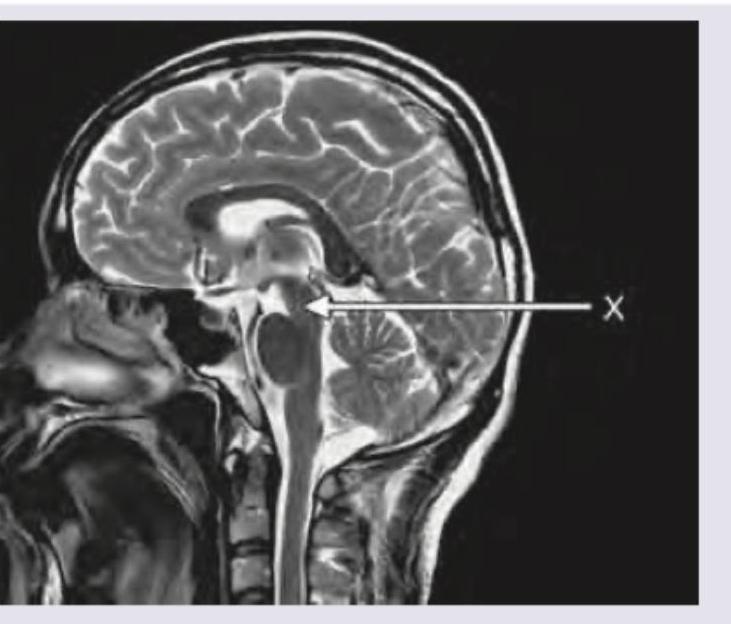
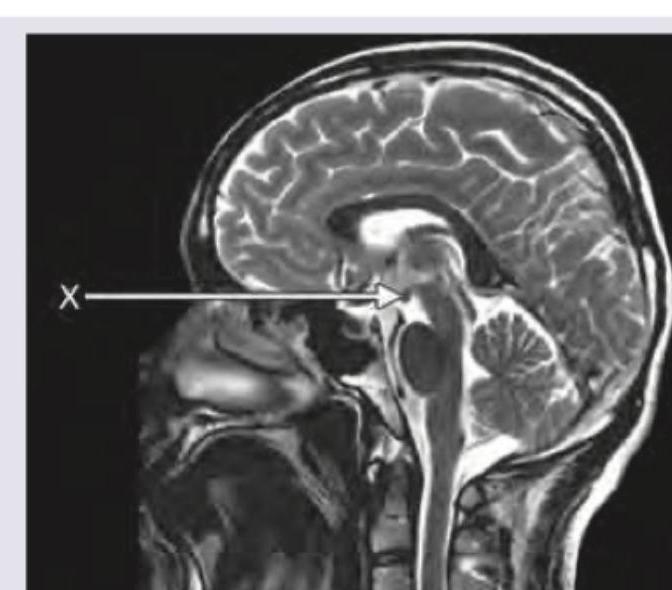
The area marked in sagittal T2-weighted MRI is?
Which is the structure marked here?
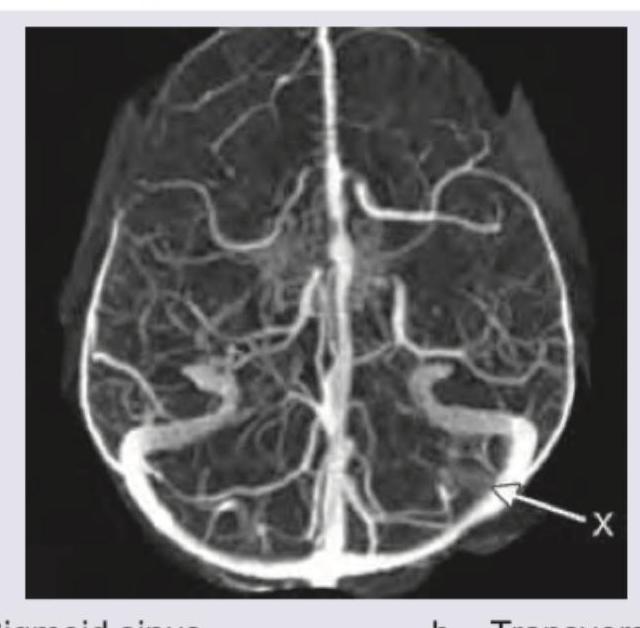
The structure marked as $X$ in the below shown MR venography of the brain is:
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app