
Brain and Neuroanatomy — MCQs

On this page
The pyramids are formed by which of the following structures?
Which intracranial structure is sensitive to pain?
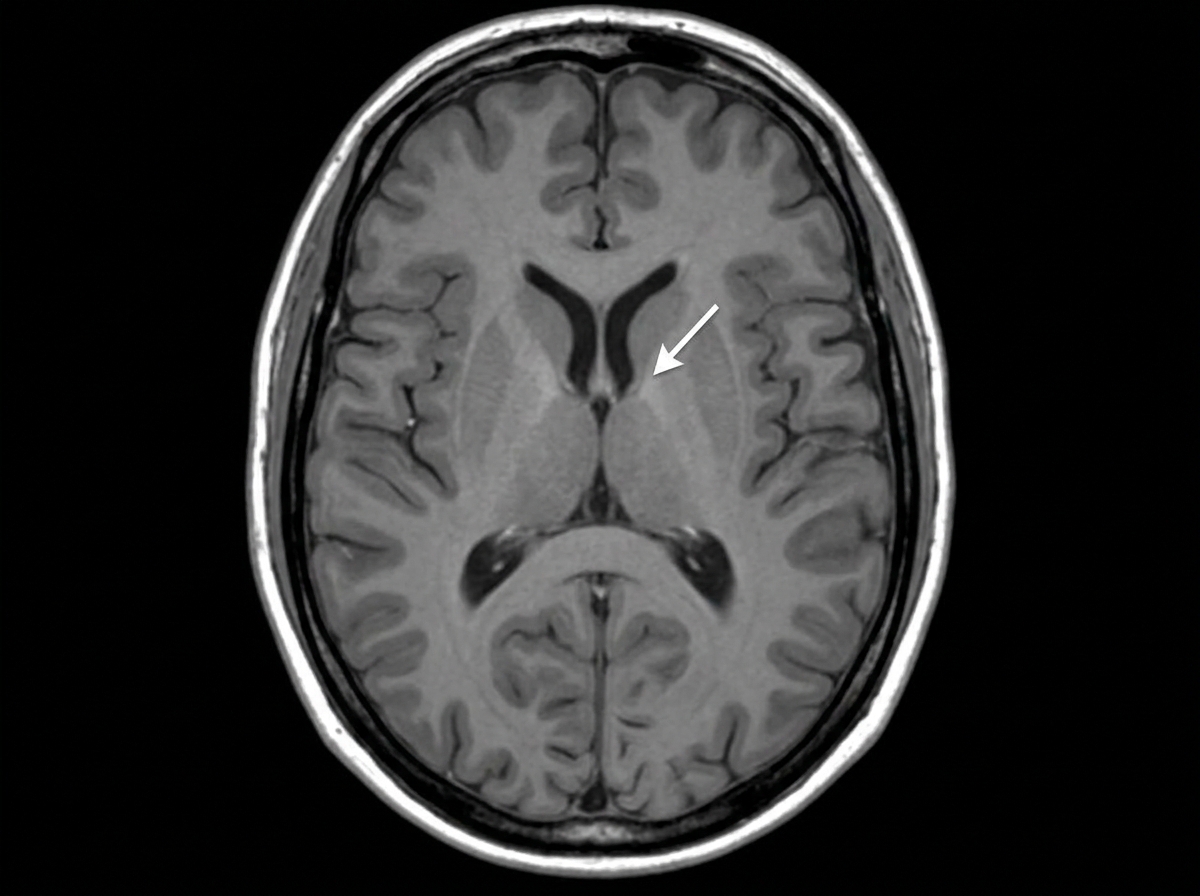
Identify the marked structure:
A subject was brought to the Casualty with a history of RTA and head injury. On examination, he was conscious. When the doctor asked questions about the incident, his answers were irrelevant to the questions, but his speech was fluent. What could be the possible site of injury?
In the sagittal section of the brain given below the colored area represents the paracentral lobule. Which of the following structures are affected in a lesion to this area?
Which nerve is not related to olfaction?
During a neck dissection, a nerve was identified and marked that is most likely the vagus nerve (CN X). Which of the following is NOT a functional component of the vagus nerve?
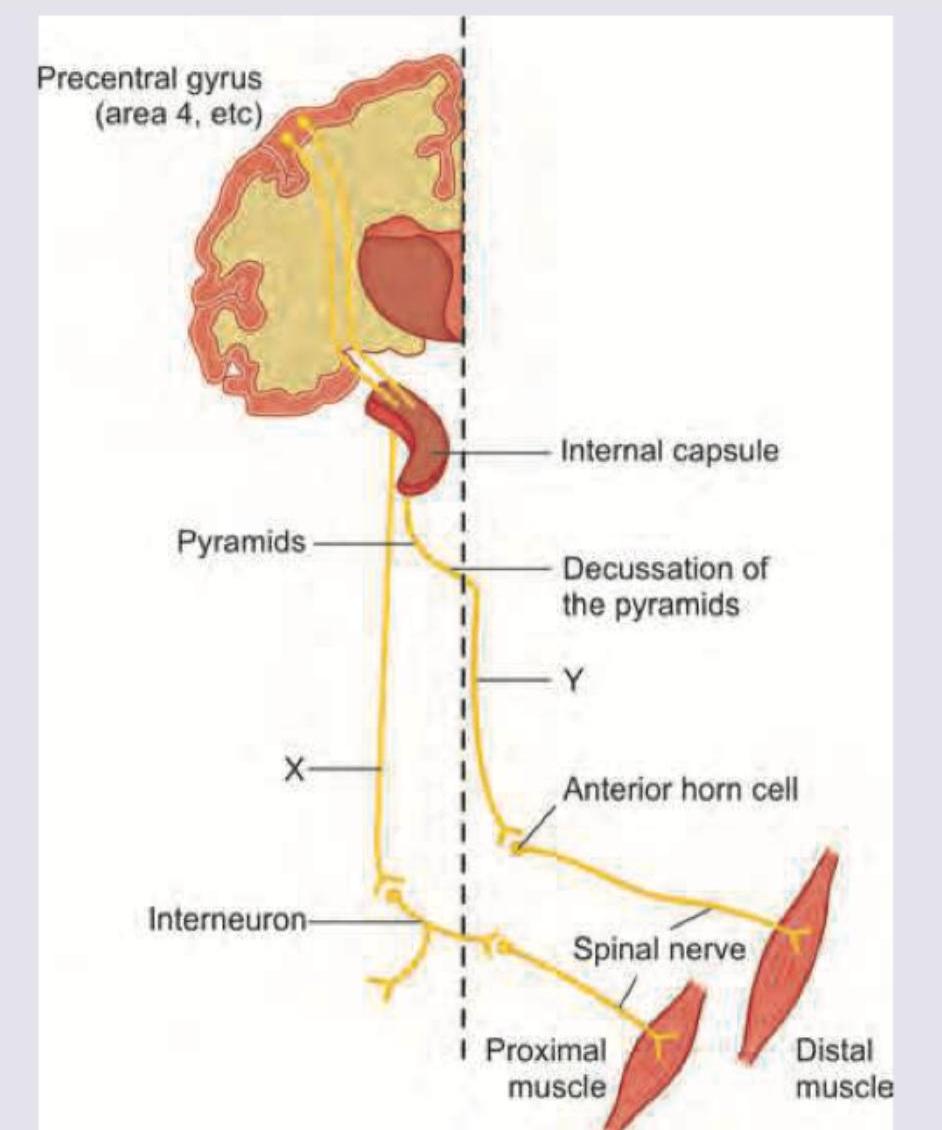
Name the pathways marked as $X$ and $Y$.
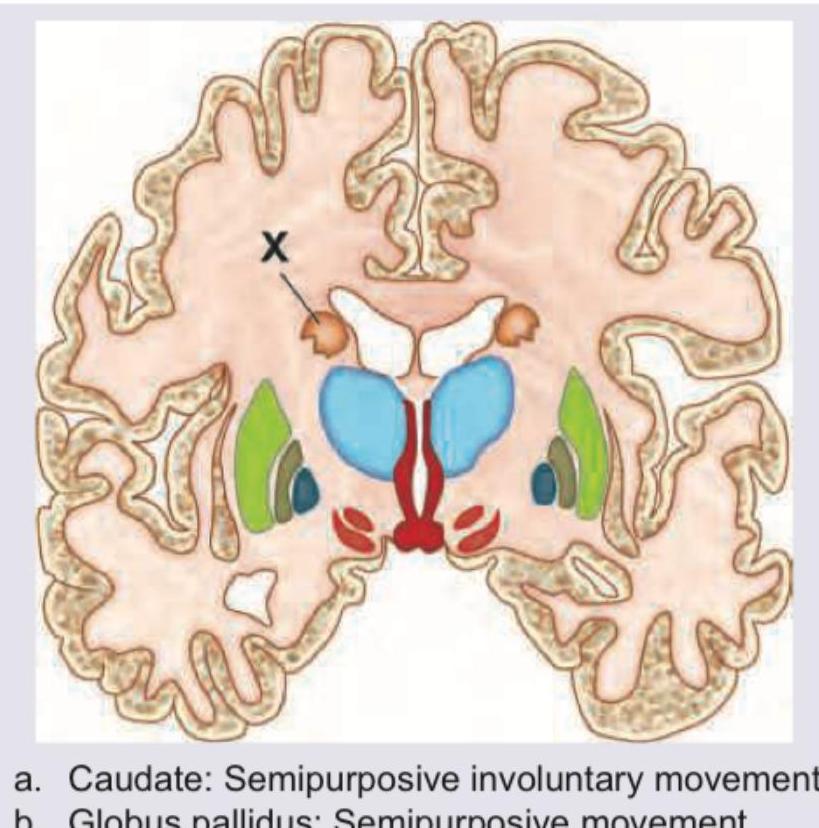
Which of the following is correct about lesion in the basal ganglia marked as $X$ and its manifestation?
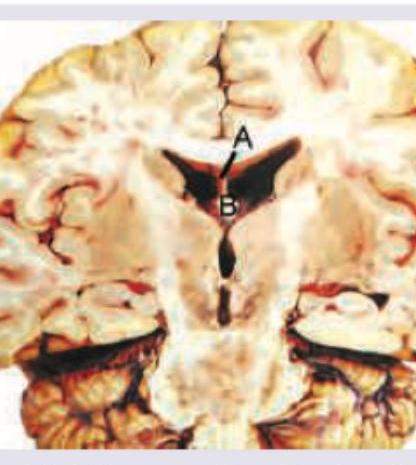
Which is correct about the image shown below?
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app