
Brain and Neuroanatomy — MCQs

On this page
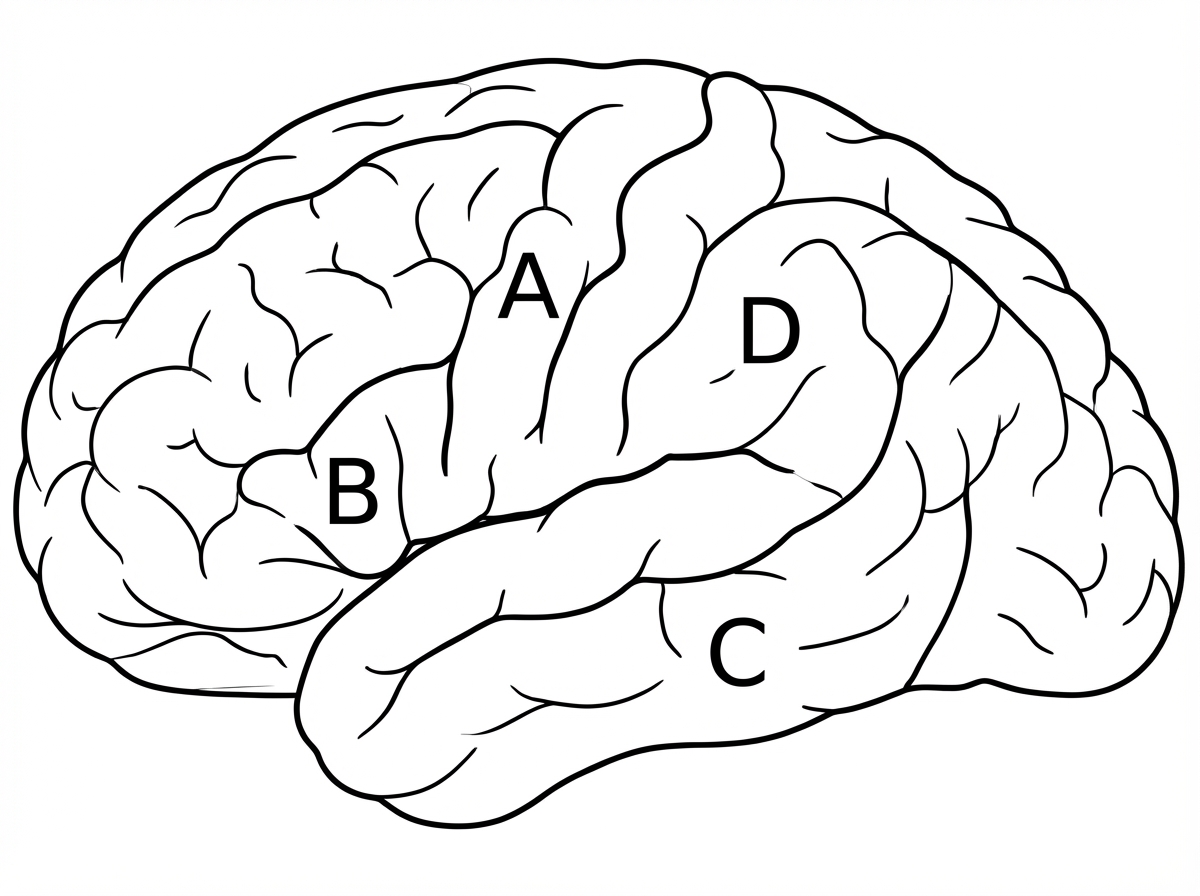
A right-hand dominant person presents with Broca's Aphasia. This is likely to result from damage to which area?
Wallenberg's syndrome may involve which of the following structures?
Which is the most common cranial nerve involved in the pathology of an intracranial aneurysm?
A 25-year-old male involved in a road traffic accident presents to the emergency department. On examination, he is alert and has nonfluent, effortful speech with preserved comprehension. Which of the following areas of the brain is most likely involved?
All of the following arteries supply the medulla oblongata, except?
The medial geniculate body is an eminence on the inferior surface of the thalamus lateral to the midbrain. Which of the following functions is related to the medial geniculate body?
Which of the following is NOT a terminal branch of the internal carotid artery?
Which of the following is NOT a branch of the internal carotid artery?
A lesion in the left optic tract typically manifests as which of the following visual field defects?
Charcot's artery is:
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app