
Brain and Neuroanatomy — MCQs

On this page
Wernicke's area is located in which part of the brain?
What is the efferent limb of the gag reflex?
What order neuron is the optic nerve?
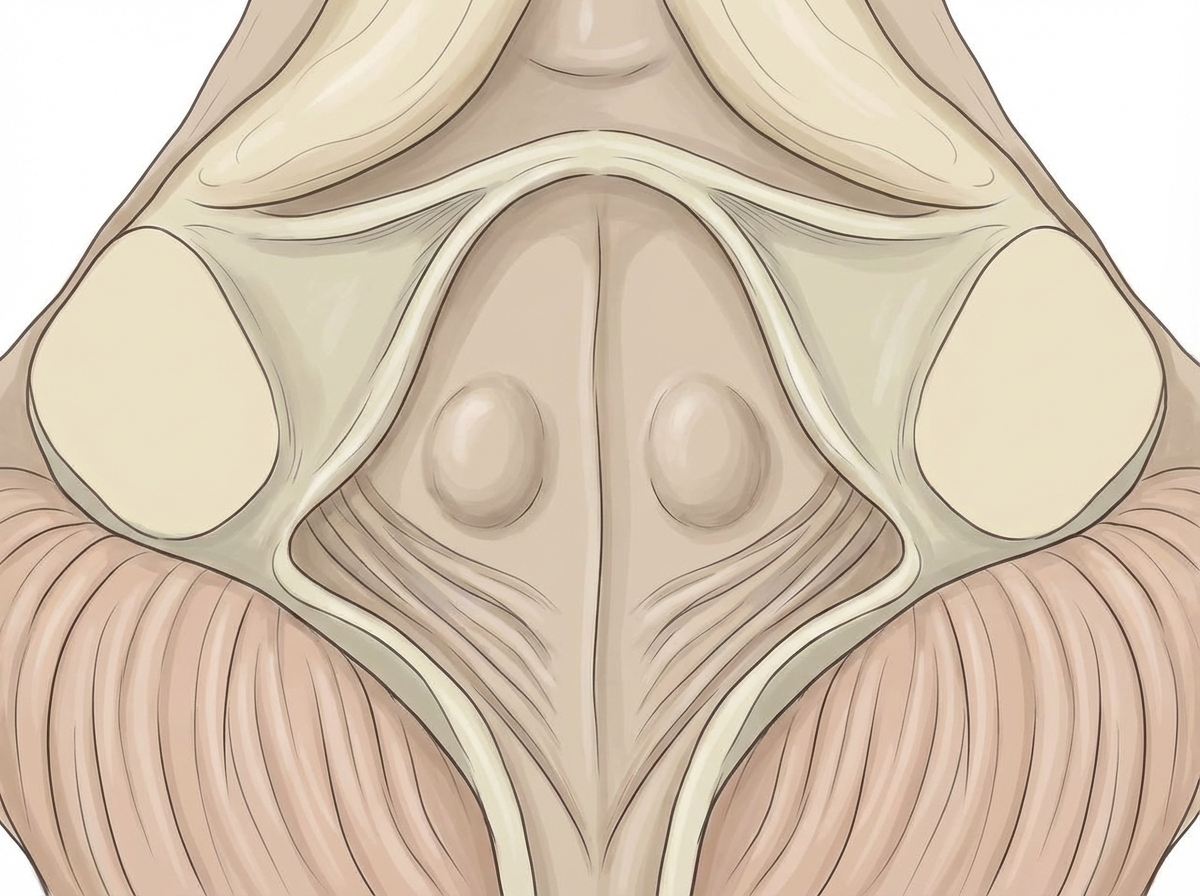
Damage to the internal genu of the facial nerve forming the marked elevation leads to paralysis of which of the following muscles?
All of the following are nuclei of the cerebellum, EXCEPT:
Which of the following statements is NOT true regarding the optic nerve?
All are common sites of berry aneurysm, EXCEPT?
Which of the following is NOT a normal variant of intracranial venous drainage?
Which Brodmann areas constitute Broca's area?
Which nuclei are located deep within the medial temporal lobes of the brain?
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app