
Brain and Neuroanatomy — MCQs

On this page
Which one of the following extraocular muscles is served by a contralateral brainstem subnucleus?
Which artery directly supplies the medial surfaces of the frontal and parietal lobes of the brain?
Association fibers include all of the following except?
Which of the following statements regarding the third cranial nerve is NOT true?
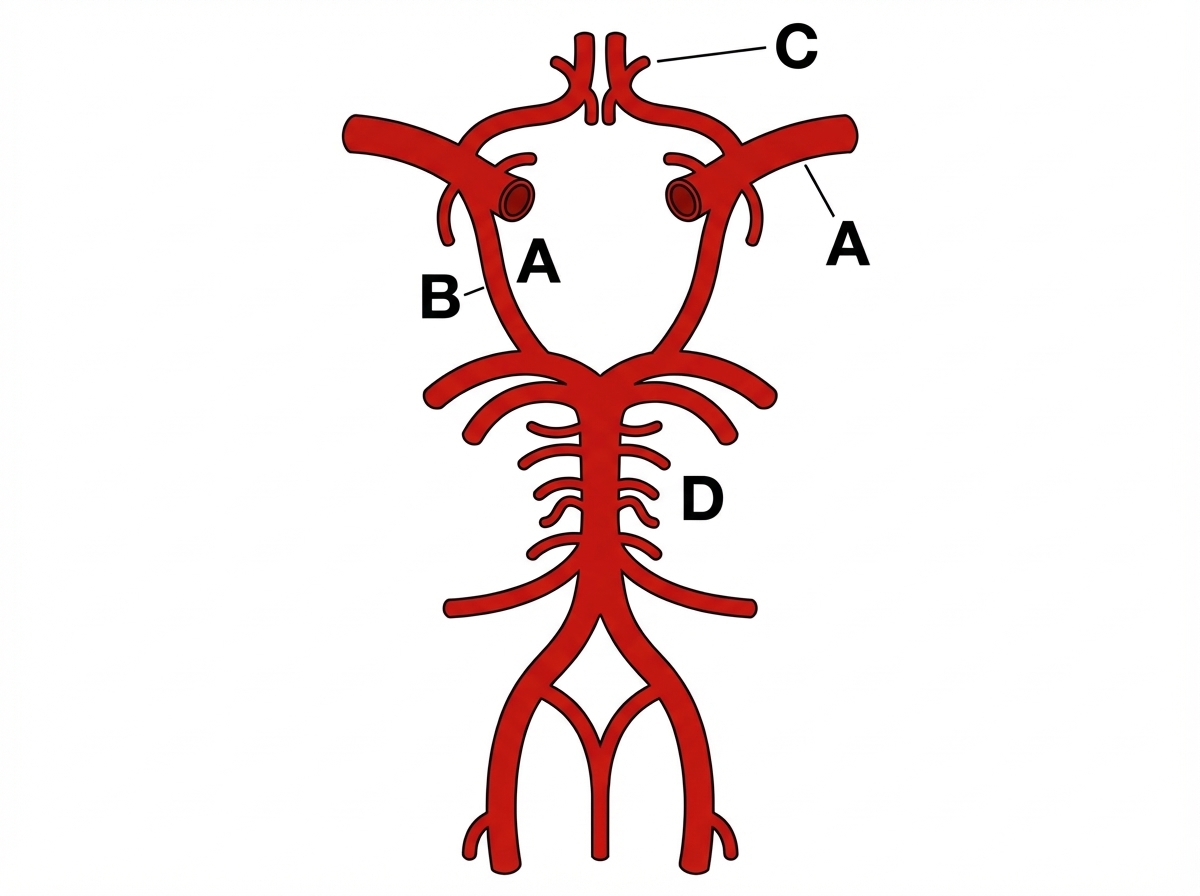
Which of the following is NOT a common site for intracranial aneurysms?
Which of the following is NOT a constituent of the inferior cerebellar peduncle?
A person has inability to look downward and laterally. Which nerve is injured?
The hypoglossal nucleus is located in which part of the brainstem?
Which of the following arteries supplies blood to the trigeminal ganglion?
Which of the following sites is not typically involved in a posterior cerebral artery infarct?
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app