
Brain and Neuroanatomy — MCQs

On this page
Which of the following statements regarding the cerebral cortex is NOT true?
Most of the afferents from the lateral geniculate body terminate in which layer of the visual cortex?
Which structure does not pass through the superior cerebellar peduncle?
Which of the following areas is located in the temporal lobe?
All of the following cortical areas contribute fibers to the corticospinal tract, EXCEPT?
The central sulcus is an example of which type of sulcus?
The primary visual area is located in the walls of which structure?
Which nerve supplies the dilator pupillae muscle?
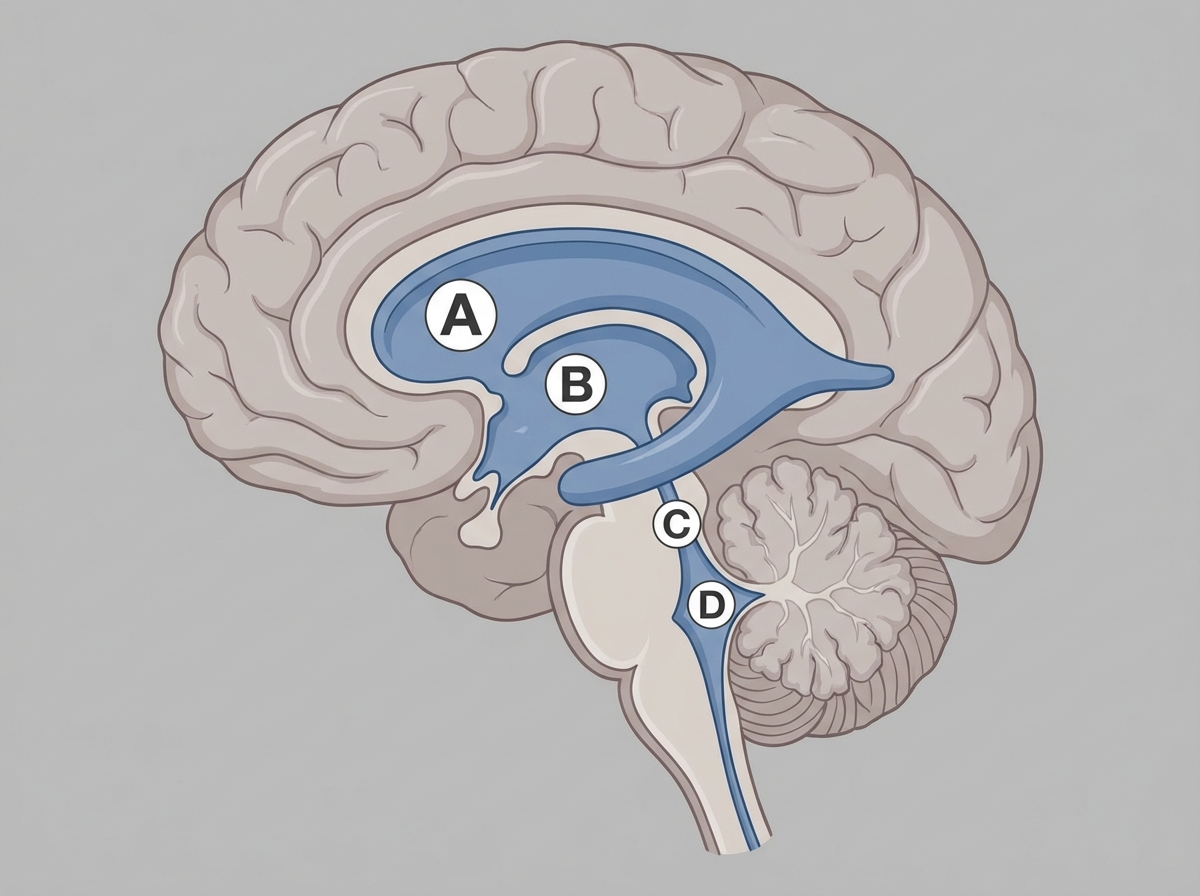
Cerebrospinal fluid is primarily produced by the choroid plexus in which structure?
Which of the following is NOT a feature found in the cerebellum?
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app