
Brain and Neuroanatomy — MCQs

On this page
What artery supplies the hippocampus?
Which Brodmann area corresponds to the premotor area?
The trochlear nerve nucleus is located at the level of which midbrain structure?
Which of the following statements is TRUE about the limbic system?
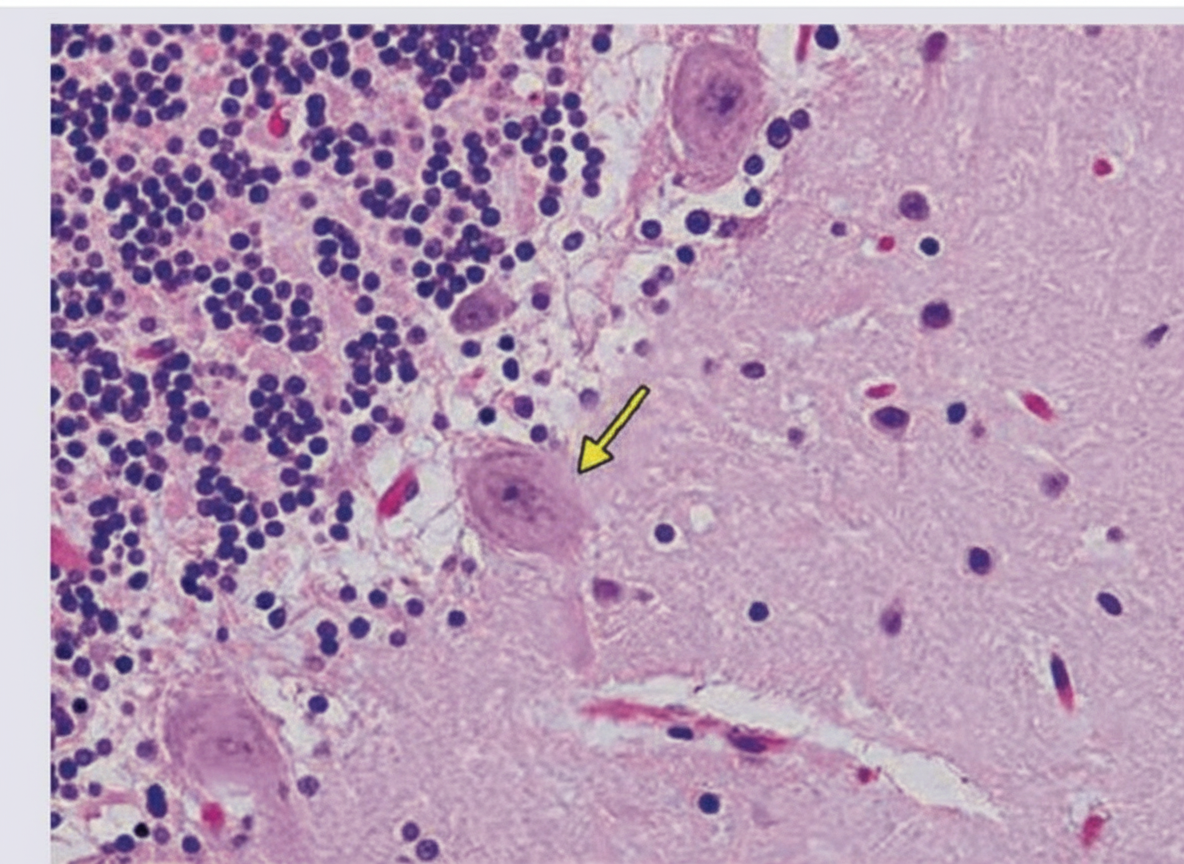
The marked cell primarily inhibits which of the following structures?
Which part of the brain contains the olivary nucleus?
Which of the following lobes of the cerebrum is related to the inferior horn of the lateral ventricle?
The superior colliculus is primarily concerned with which function?
All of the following are included under basal ganglia except?
Substantia gelatinosa corresponds to which of Rexed's laminae?
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app