
Brain and Neuroanatomy — MCQs

On this page
Identify the marked structure.
Identify the marked structure:
Which artery supplies the deep cerebellar nuclei?
Which thalamic nucleus projects to the striatum?
Which of the following is NOT a branch of the basilar artery?
What is true about the Vein of Labbe?
A 9-year-old boy is diagnosed with multiple sclerosis (MS). Which of the following nervous structures would most likely be affected by this disease?
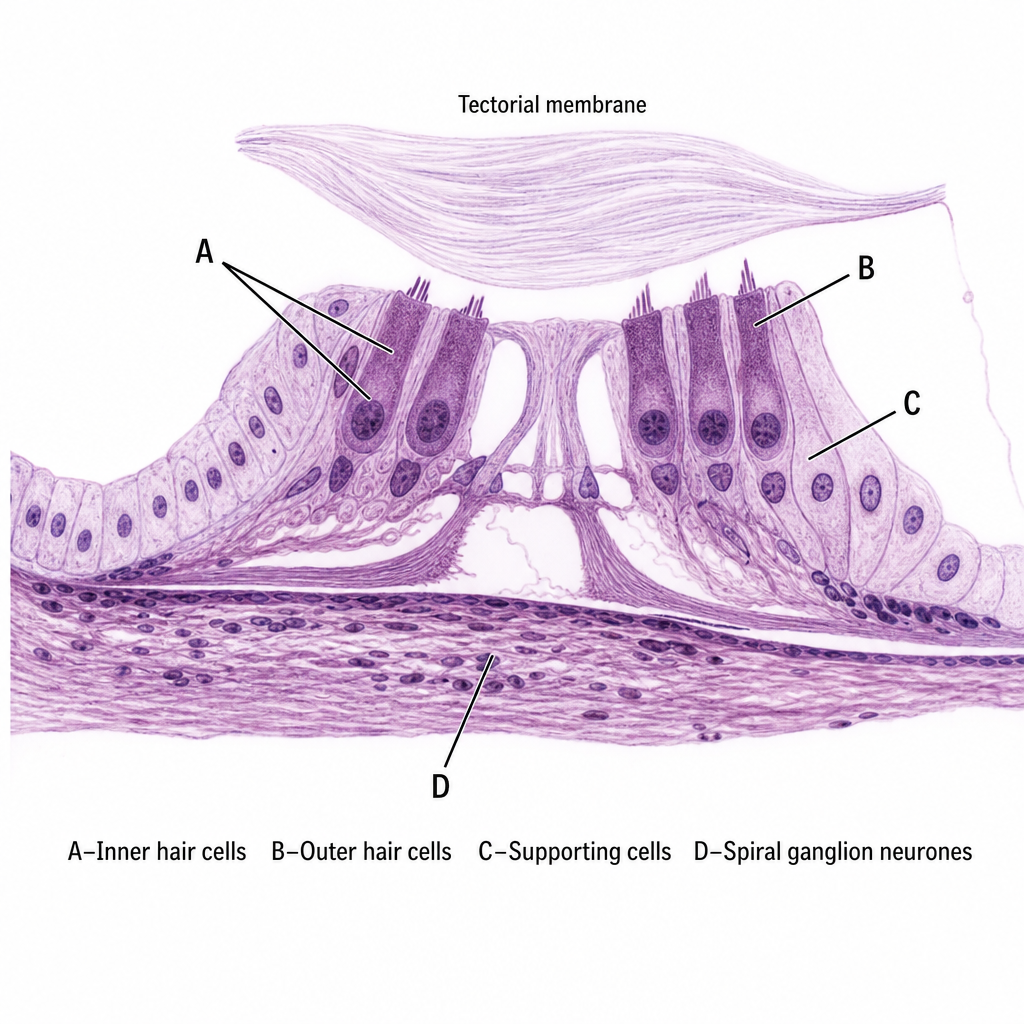
The spiral ganglion innervates which of the following cells shown in the diagram?
Which of the following supplies the pineal gland?
Which venous sinus is present over the falx cerebelli?
Practice by Chapter
Cerebral Hemispheres
Practice Questions
Diencephalon
Practice Questions
Brainstem
Practice Questions
Cerebellum
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Ventricular System and CSF
Practice Questions
Blood Supply of the Brain
Practice Questions
Cranial Nerves and Nuclei
Practice Questions
Functional Systems and Pathways
Practice Questions
Applied Neuroanatomy
Practice Questions
Neuroimaging Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app