UPSC-CMS 2012 — Internal Medicine
7 Previous Year Questions with Answers & Explanations
The commonest cause of primary hyper-parathyroidism is
In a 30-year-old male smoker, the commonest cause of dry gangrene of foot will be
The Ranson prognostic criteria used at the time of admission in acute pancreatitis include all of the following except
The most common opportunistic infection observed in patients with AIDS is
Which of the following conditions may produce "wrist drop" ?
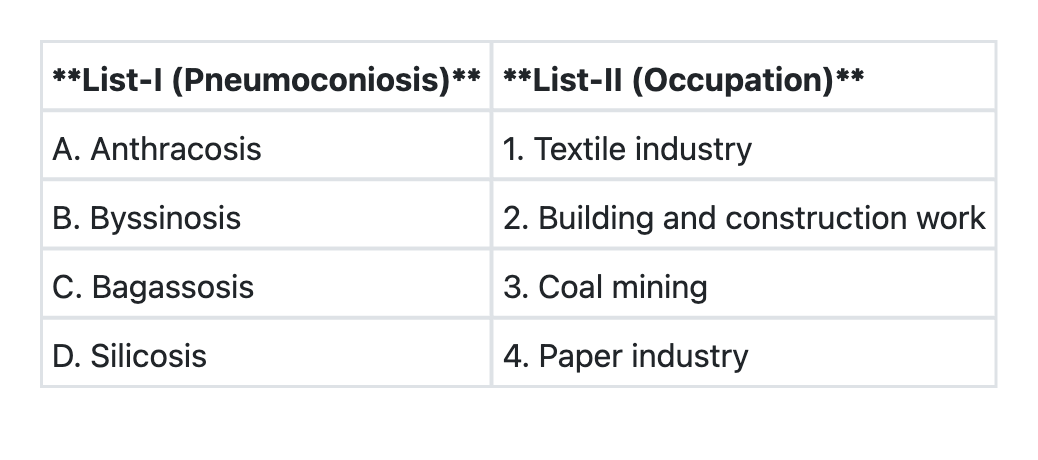
Match List-I with List-II and select the correct answer using the code given below the Lists:
Which of the following is a non-modifiable risk factor for coronary heart disease ?
UPSC-CMS 2012 - Internal Medicine UPSC-CMS Practice Questions and MCQs
Question 1: The commonest cause of primary hyper-parathyroidism is
- A. Idiopathic parathyroid hyperplasia
- B. Familial hyperparathyroidism
- C. Primary parathyroid carcinoma
- D. Parathyroid adenoma (Correct Answer)
Explanation: ***Parathyroid adenoma*** - **Parathyroid adenomas** account for approximately **85% of all cases** of primary hyperparathyroidism. [1] - This condition involves a **benign tumor** of one or more parathyroid glands that secretes excessive parathyroid hormone (PTH), leading to hypercalcemia. [1] *Idiopathic parathyroid hyperplasia* - **Idiopathic parathyroid hyperplasia** is responsible for about **10-15% of cases** of primary hyperparathyroidism, making it less common than adenomas. - In hyperplasia, **all four parathyroid glands** are typically enlarged and overactive, unlike the localized growth in an adenoma. *Familial hyperparathyroidism* - **Familial hyperparathyroidism** is a rare cause, accounting for **less than 1% of cases**, and is often associated with genetic syndromes like **MEN1** or **MEN2A**. - It involves inherited genetic mutations that predispose individuals to parathyroid gland overactivity, which distinguishes it from sporadic causes. *Primary parathyroid carcinoma* - **Primary parathyroid carcinoma** is an **extremely rare malignancy**, accounting for **less than 1%** of all primary hyperparathyroidism cases. - While it causes severe hypercalcemia, its rarity means it is not the commonest cause.
Question 2: In a 30-year-old male smoker, the commonest cause of dry gangrene of foot will be
- A. Diabetes mellitus
- B. Embolism
- C. Atherosclerosis
- D. Buerger's disease (Correct Answer)
Explanation: Buerger's disease - **Buerger's disease** (**thromboangiitis obliterans**) is strongly associated with **heavy smoking** and typically affects young to middle-aged adult males, leading to dry gangrene in the extremities. - It involves **inflammation and thrombosis** of small and medium-sized arteries and veins, predominantly in the limbs, often manifesting as **ischemic pain**, ulcerations, and gangrene. *Diabetes mellitus* - While **diabetes** can cause dry gangrene due to **peripheral artery disease** and small vessel disease, it is more commonly associated with **wet gangrene** due to increased infection risk, and the age and smoking history point away from it being the *commonest* cause in this specific demographic for dry gangrene [1]. - Diabetic neuropathy can also mask symptoms, leading to delayed presentation and worsening tissue damage [1]. *Embolism* - An **embolic event** would typically present with **sudden onset** severe pain, pallor, pulselessness, paresthesia, and paralysis (the "6 Ps"), leading to acute limb ischemia rather than the progressive dry gangrene described implied in the question. - While it can cause tissue necrosis, it's usually an acute event rather than a chronic process leading to gradual gangrene. *Atherosclerosis* - While **atherosclerosis** is a significant cause of peripheral artery disease and gangrene, especially in smokers, it typically affects an **older population** than the 30-year-old male described [2]. - In younger smokers with gangrene, **Buerger's disease** is a more specific and common diagnosis, as atherosclerosis tends to manifest later in life unless other significant risk factors are present [2].
Question 3: The Ranson prognostic criteria used at the time of admission in acute pancreatitis include all of the following except
- A. Blood glucose more than 200 mg/100 mL
- B. WBC count more than 16,000/mm3
- C. Serum calcium < 2.0 mmol/L (Correct Answer)
- D. Age more than 55 years
Explanation: ***Serum calcium < 2.0 mmol/L*** - This option refers to a low serum calcium level, which is part of the **Ranson criteria measured 48 hours after admission**, not at admission. - The initial Ranson criteria (on admission) focus on demographic and immediate lab results. *Blood glucose more than 200 mg/100 mL* - An elevated **blood glucose > 200 mg/100 mL** is one of the five Ranson criteria assessed at the time of admission. - High glucose indicates significant physiological stress and typically a more severe illness. *WBC count more than 16,000/mm3* - An elevated **white blood cell count > 16,000/mm3** is one of the Ranson criteria assessed at admission. - This indicates a significant inflammatory response, suggesting severe pancreatitis. *Age more than 55 years* - **Age > 55 years** is one of the Ranson criteria assessed at the time of admission [1]. - Older age is a recognized risk factor for more severe outcomes in acute pancreatitis [1].
Question 4: The most common opportunistic infection observed in patients with AIDS is
- A. Pseudomonas aeruginosa
- B. Atypical mycobacteria
- C. Haemophilus influenzae
- D. Pneumocystis carinii (Correct Answer)
Explanation: ***Pneumocystis carinii*** - **Pneumocystis pneumonia (PCP)**, caused by *Pneumocystis jirovecii* (formerly *P. carinii*), is the **most common opportunistic infection** and a leading cause of death in AIDS patients [1]. - It typically presents with **fever, cough, and dyspnea** in patients with a CD4 count below 200 cells/µL [1]. *Pseudomonas aeruginosa* - While *Pseudomonas aeruginosa* can cause serious infections in immunocompromised individuals, it is not the **most common opportunistic infection** seen in patients with AIDS. - Infections usually involve the **lungs (pneumonia)**, skin, urinary tract, or bacteremia, often in patients with **neutropenia** or hospitalized for other reasons. *Atypical mycobacteria* - **Mycobacterium avium complex (MAC)** is an important opportunistic pathogen in AIDS patients (CD4 < 50 cells/µL), causing disseminated disease, but it is not the **most common** overall [2]. - Symptoms include **fever, weight loss, night sweats, and diarrhea**, and diagnosis requires blood cultures or tissue biopsy [2]. *Haemophilus influenzae* - *Haemophilus influenzae* can cause **respiratory tract infections** (e.g., sinusitis, bronchitis, pneumonia) and invasive disease, particularly in children and individuals with underlying lung disease. - While patients with HIV may be more susceptible to bacterial infections, *H. influenzae* is **not classified as a classic opportunistic infection** in the same way as *Pneumocystis* or MAC in AIDS patients.
Question 5: Which of the following conditions may produce "wrist drop" ?
- A. Alcoholics
- B. Beriberi
- C. Lead poisoning (Correct Answer)
- D. Diabetes mellitus
Explanation: ***Lead poisoning*** - **Lead neuropathy** predominantly affects motor nerves, often leading to **wrist drop** and **foot drop** due to involvement of the radial and peroneal nerves, respectively [1]. - The toxic effects of lead interfere with heme synthesis and neuronal function, leading to **demyelination** and axonal degeneration [1]. *Alcoholics* - **Alcoholic neuropathy** typically affects peripheral nerves, causing sensory and motor deficits, often as a **stocking-glove distribution** [3]. - While it can manifest as weakness, classic "wrist drop" is not a hallmark feature; rather, it often involves generalized weakness and sensory loss. *Beriberi* - **Beriberi** is caused by **thiamine (vitamin B1) deficiency** and presents in two main forms: wet (cardiovascular) and dry (neurological). - Dry beriberi causes **peripheral neuropathy** with symmetrical motor and sensory impairment, but **wrist drop** is not a characteristic isolated sign. *Diabetes mellitus* - **Diabetic neuropathy** commonly leads to a **stocking-glove sensory loss** and - Can cause motor weakness, but isolated **wrist drop** [2] is not a typical presentation; rather, it's often polyneuropathy or mononeuropathy multiplex [3].
Question 6: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→3 B→1 C→2 D→4 (Correct Answer)
- B. A→3 B→2 C→1 D→4
- C. A→1 B→4 C→2 D→3
- D. A→4 B→2 C→1 D→3
Explanation: ***A→3 B→1 C→2 D→4*** - This option correctly matches each pneumoconiosis with its associated occupation. - **Anthracosis** is linked to coal mining, **Byssinosis** to the textile industry, **Bagassosis** to the paper industry, and **Silicosis** to building and construction work. *A→3 B→2 C→1 D→4* - This option incorrectly matches **Byssinosis** with building and construction work and **Bagassosis** with the textile industry. - Byssinosis is caused by cotton dust in the textile industry, and Bagassosis is caused by bagasse dust, commonly from the sugar cane or paper industry. *A→1 B→4 C→2 D→3* - This option contains multiple incorrect matches, including linking Anthracosis to the textile industry and Silicosis to coal mining. - Anthracosis is specifically tied to **coal dust exposure**, and Silicosis results from **silica dust inhalation**. *A→4 B→2 C→1 D→3* - This option is incorrect because it mismatches Anthracosis with the paper industry and Bagassosis with the textile industry, among others. - Each pneumoconiosis has a distinct occupational exposure source.
Question 7: Which of the following is a non-modifiable risk factor for coronary heart disease ?
- A. Elevated serum cholesterol
- B. Age (Correct Answer)
- C. Alcoholism
- D. Cigarette smoking
Explanation: ***Age*** - Age is a **non-modifiable risk factor** for coronary heart disease because it cannot be changed or controlled. As people age, their risk of developing CHD naturally increases due to physiological changes and increased exposure to other risk factors over time. [1] - The older an individual is, especially for men over 45 and women over 55, the higher their risk for developing **atherosclerosis** and its complications, including CHD. [1] *Elevated serum cholesterol* - **Elevated serum cholesterol**, particularly high levels of LDL cholesterol, is a **modifiable risk factor** because it can be lowered through diet, exercise, and medication. [1] - Reducing cholesterol levels can significantly decrease the risk of **atherosclerosis** and subsequent CHD. [1] *Alcoholism* - **Alcoholism** is a **modifiable risk factor** as it represents a lifestyle choice that can be changed through behavioral interventions and support. - Excessive alcohol consumption can contribute to high blood pressure, **cardiomyopathy**, and increased triglyceride levels, all of which raise the risk of CHD. *Cigarette smoking* - **Cigarette smoking** is a major **modifiable risk factor** for CHD because it is a habit that individuals can choose to stop. [1] - Smoking damages blood vessels, increases **blood clotting**, and reduces oxygen delivery to the heart, significantly accelerating the development of atherosclerosis. [1]