UPSC-CMS 2010 — Pathology
8 Previous Year Questions with Answers & Explanations
Hypertrophic scar is characterized by the following, except
Langhans' giant cells are characteristically seen in
Acinic cell carcinoma is found in
Which one of the following is not a premalignant condition for colon cancer?
Osteitis fibrosa cystica is a feature of
Match List-I with List-II and select the correct answer using the code given below the Lists:
Which one of the following is due to the monosomy of X-chromosome?
Which tumour marker is most often elevated in ovarian granulosa cell tumour?
UPSC-CMS 2010 - Pathology UPSC-CMS Practice Questions and MCQs
Question 1: Hypertrophic scar is characterized by the following, except
- A. it involves the flexor surface
- B. it outgrows the wound area (Correct Answer)
- C. it is non-familial
- D. it is not related to the race
Explanation: ***it outgrows the wound area*** - This statement is characteristic of a **keloid scar**, not a hypertrophic scar. Keloids are distinguished by their growth beyond the original wound margins [1]. - **Hypertrophic scars**, on the other hand, remain confined within the boundaries of the original injury, though they may be raised and erythematous [1]. *it involves the flexor surface* - While hypertrophic scars can occur on any body surface, they are commonly found on areas of **high tension**, such as the **flexor surfaces** of joints (e.g., knee, elbow) or the chest and shoulders. - This involvement is due to constant movement stretching the healing skin, which can stimulate excessive collagen production. *it is non-familial* - Hypertrophic scars are generally **not associated with a strong genetic predisposition** or familial inheritance patterns. - Their development is primarily linked to factors like wound tension, infection, and individual healing responses rather than inherited tendencies. *it is not related to the race* - The incidence of hypertrophic scars does **not show a significant racial predilection**, unlike keloid scars, which are more common in individuals with darker skin types. - Hypertrophic scars can affect individuals from all racial backgrounds. **References:** [1] Kumar v, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Inflammation and Repair, pp. 119-121.
Question 2: Langhans' giant cells are characteristically seen in
- A. typhoid Peyer's patch
- B. peritoneal tuberculosis (Correct Answer)
- C. tuberculoma
- D. lymphoma
Explanation: ***Peritoneal tuberculosis*** - **Langhans' giant cells** are a characteristic histological feature of **granulomatous inflammation**, particularly seen in **tuberculosis** [1], [2]. - They are formed by the fusion of epithelioid histiocytes and are a hallmark of **mycobacterial infections**, including peritoneal tuberculosis [2]. - While not pathognomonic, their presence in the appropriate clinical context strongly suggests tuberculosis [1]. *Typhoid Peyer's patch* - **Typhoid fever** causes **macrophage infiltration** with **necrosis** and **ulceration** in Peyer's patches. - The inflammatory response is mononuclear but does **not** form **epithelioid granulomas** or Langhans' giant cells. - Histology shows mononuclear cell infiltration and typhoid nodules, not granulomatous inflammation. *Tuberculoma* - A **tuberculoma** is a localized form of tuberculosis and **also contains Langhans' giant cells** within its granulomatous structure [1]. - However, peritoneal tuberculosis represents a broader clinical entity where identification of these cells in peritoneal tissue/fluid is diagnostically significant. - Both are forms of TB, but the question context favors the systemic/cavity involvement over a localized mass lesion. *Lymphoma* - **Lymphoma** shows malignant proliferation of lymphoid cells with effacement of normal architecture. - It does **not** show **granulomatous inflammation** or Langhans' giant cells. - Histology reveals sheets of atypical lymphoid cells, not epithelioid granulomas. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Infectious Diseases, pp. 383-384. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Inflammation and Repair, p. 109.
Question 3: Acinic cell carcinoma is found in
- A. salivary glands (Correct Answer)
- B. breast
- C. thyroid
- D. stomach
Explanation: ***salivary glands*** - **Acinic cell carcinoma** is a rare malignant tumor that primarily arises in the **major salivary glands**, most commonly the **parotid gland** [1]. - Its name derives from its histologic resemblance to **serous acinar cells**, which are characteristic of salivary gland tissue. *breast* - While various carcinomas occur in the breast, **acinic cell carcinoma** is not a primary breast cancer type [2]. - Breast cancers originate from **ductal** or **lobular epithelial cells** [2]. *thyroid* - Thyroid cancers include **papillary**, **follicular**, **medullary**, and **anaplastic carcinomas**, which originate from thyroid follicular or parafollicular cells. - **Acinic cell carcinoma** is not a recognized type of thyroid malignancy. *stomach* - The stomach is susceptible to **adenocarcinomas**, particularly **intestinal** and **diffuse types**, as well as other less common tumors. - **Acinic cell carcinoma** is not found as a primary tumor in the stomach. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Head and Neck, pp. 753-755. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Breast, pp. 1059-1060.
Question 4: Which one of the following is not a premalignant condition for colon cancer?
- A. Ulcerative colitis
- B. Villous adenoma
- C. Familial adenomatous polyposis coli
- D. Sporadic hamartomatous polyps (Correct Answer)
Explanation: ***Sporadic hamartomatous polyps*** - **Sporadic hamartomatous polyps** are benign lesions composed of normal tissue elements arranged in a disorganized manner and do not carry significant risk of malignant transformation. - Unlike adenomatous polyps, sporadic hamartomatous polyps lack **dysplastic epithelium** and are not considered premalignant [2]. - **Important distinction:** While **hamartomatous polyposis syndromes** (e.g., Peutz-Jeghers syndrome, Juvenile polyposis syndrome) do increase cancer risk due to the large number of polyps and associated genetic mutations, individual sporadic hamartomatous polyps themselves are not premalignant [3]. *Ulcerative colitis* - **Ulcerative colitis** is a chronic inflammatory bowel disease that significantly increases the risk of developing colorectal cancer, especially with long-standing disease (>8-10 years) or extensive colonic involvement. - The chronic inflammation leads to **dysplasia**, which is a precursor to malignancy, making it a true premalignant condition. *Villous adenoma* - **Villous adenomas** are a type of adenomatous polyp with the highest propensity for malignant transformation (30-40% harbor carcinoma) [4]. - They have a characteristic finger-like villous architecture and often contain **high-grade dysplasia**, significantly increasing the likelihood of progression to invasive carcinoma [1], [4]. *Familial adenomatous polyposis coli* - **Familial adenomatous polyposis (FAP)** is an autosomal dominant disorder caused by **APC gene mutation**, characterized by the development of hundreds to thousands of adenomatous polyps throughout the colon and rectum [2]. - Nearly **100% of individuals with untreated FAP** will develop colorectal cancer by age 40, making it one of the most highly penetrant premalignant conditions [2]. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Alimentary System Disease, pp. 371-372. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Gastrointestinal Tract, pp. 821-822. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Gastrointestinal Tract, pp. 813-814. [4] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Gastrointestinal Tract, pp. 815-817.
Question 5: Osteitis fibrosa cystica is a feature of
- A. milk-alkali syndrome
- B. rickets
- C. hyperthyroidism
- D. hyperparathyroidism (Correct Answer)
Explanation: ***Correct: Hyperparathyroidism*** - **Osteitis fibrosa cystica** is a classic bone manifestation of **severe primary hyperparathyroidism**, resulting from excessive **parathyroid hormone (PTH)** [1]. - **PTH** causes increased bone resorption, leading to fibrous tissue replacement, cystic changes, and **brown tumors** (osteoclast-rich lesions with hemosiderin deposition) [1], [2]. - This represents advanced skeletal disease in hyperparathyroidism, though now rare due to early detection [1]. *Incorrect: Milk-alkali syndrome* - This syndrome is characterized by **hypercalcemia**, **metabolic alkalosis**, and **renal insufficiency** due to excessive intake of calcium and absorbable alkali. - It does not cause osteitis fibrosa cystica, which is a specific bone lesion requiring prolonged elevated **PTH**. *Incorrect: Rickets* - **Rickets** is a disorder primarily affecting children, characterized by defective bone mineralization leading to soft and weakened bones. - It is caused by **vitamin D deficiency** or resistance and manifests as bone deformities (bowing, rachitic rosary), not cystic bone lesions. *Incorrect: Hyperthyroidism* - **Hyperthyroidism** can lead to generalized **osteopenia** or **osteoporosis** due to increased bone turnover, but it does not cause osteitis fibrosa cystica. - The bone changes in hyperthyroidism are diffuse and distinct from the focal cystic lesions seen in excessive **PTH** activity. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1105-1106. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Bones, Joints, and Soft Tissue Tumors, p. 1194.
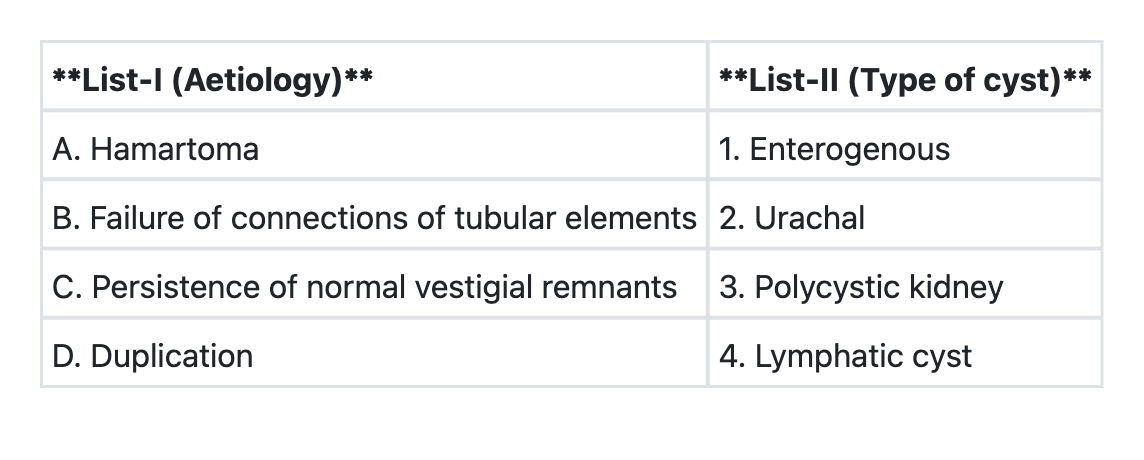
Question 6: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→3 B→4 C→1 D→2
- B. A→4 B→3 C→2 D→1 (Correct Answer)
- C. A→3 B→1 C→4 D→2
- D. A→2 B→4 C→1 D→3
Explanation: ***A→4 B→3 C→2 D→1*** - A **hamartoma** is a benign, focal malformation resembling a neoplasm, composed of mature cells and tissues normally found in the organ from which it arises, but growing in a disorganized mass. A **lymphatic cyst** (or lymphangioma/cystic hygroma), though often confused with a true neoplasm, is a congenital malformation of the lymphatic system, a type of hamartoma [1]. - **Polycystic kidney disease** is characterized by the formation of numerous cysts in the kidneys. One of the theories for its pathogenesis involves the failure of connections between collecting tubules and nephrons during renal development, leading to isolated segments that dilate to form cysts [2], [3]. - The **urachus** is an embryonic remnant of the allantois, connecting the fetal bladder to the umbilicus. If the urachus fails to involute completely after birth, it can persist as a patent or partially patent structure, leading to various **urachal anomalies**, including urachal cysts. - **Duplication** can lead to the formation of an **enterogenous cyst**, which is a congenital cyst lined by typical gastrointestinal mucosa. These cysts arise from developmental errors during embryogenesis where portions of the primitive gut tube become duplicated or sequestered. *A→3 B→4 C→1 D→2* - This option incorrectly associates hamartoma with polycystic kidney and duplication with urachal cysts. - **Polycystic kidney** is primarily due to defects in tubular connections, not hamartomas, and **urachal cysts** are remnants of vestigial structures, not duplications. *A→3 B→1 C→4 D→2* - This option incorrectly associates hamartoma with polycystic kidney and persistence of normal vestigial remnants with lymphatic cyst. - **Polycystic kidney** is not a hamartoma, and **lymphatic cysts** are not typical vestigial remnants but rather developmental malformations of the lymphatic system [1]. *A→2 B→4 C→1 D→3* - This option incorrectly associates hamartoma with urachal cysts and persistence of normal vestigial remnants with enterogenous cysts. - **Urachal cysts** are vestigial remnants, not hamartomas. **Enterogenous cysts** are a result of duplication, not persistence of normal vestigial remnants. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of Infancy and Childhood, pp. 481-482. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 544-545. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, pp. 951-952.
Question 7: Which one of the following is due to the monosomy of X-chromosome?
- A. Klinefelter's syndrome
- B. Turner's syndrome (Correct Answer)
- C. Testicular feminization
- D. Adrenogenital syndrome
Explanation: ***Turner's syndrome*** - Turner's syndrome is characterized by the **monosomy of the X chromosome** (genotype 45, XO), meaning an individual has only one X chromosome instead of the usual two [4]. - This chromosomal abnormality leads to a range of developmental issues, primarily affecting females, including **short stature**, **ovarian dysgenesis**, and a **webbed neck** [2]. *Klinefelter's syndrome* - This syndrome is due to the presence of an **extra X chromosome in males** (genotype 47, XXY), not a monosomy [1]. - It typically results in **testicular atrophy**, **gynecomastia**, and **tall stature** [1]. *Testicular feminization* - Also known as **Androgen Insensitivity Syndrome (AIS)**, this is a **genetic disorder** where individuals with XY chromosomes are unable to respond to androgens [3]. - It results in the development of female external genitalia, but it is due to a **receptor defect**, not a chromosomal monosomy [3]. *Adrenogenital syndrome* - This is primarily caused by **congenital adrenal hyperplasia (CAH)**, a group of genetic disorders affecting the adrenal glands' hormone production. - It is an **autosomal recessive disorder** involving enzyme deficiencies in cortisol synthesis, not a chromosomal monosomy. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, pp. 174-175. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, pp. 175-177. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 93-94. [4] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, pp. 173-174.
Question 8: Which tumour marker is most often elevated in ovarian granulosa cell tumour?
- A. Alpha fetoprotein
- B. CA 125
- C. Inhibin (Correct Answer)
- D. Beta-HCG
Explanation: ***Inhibin*** - **Inhibin** is a polypeptide hormone produced by granulosa cells, making it a highly specific and sensitive marker for **granulosa cell tumors** of the ovary [1]. - Its levels correlate with tumor burden and can be used for monitoring treatment response and detecting recurrence [1]. *Alpha fetoprotein* - **Alpha-fetoprotein (AFP)** is a tumor marker more commonly associated with **yolk sac tumors (endodermal sinus tumors)**, which are a type of germ cell tumor, not granulosa cell tumors. - Elevated AFP can also be seen in hepatocellular carcinoma and some testicular tumors. *CA 125* - **CA 125** is the most widely used tumor marker for **epithelial ovarian cancer**, which is the most common type of ovarian cancer. - While it can be mildly elevated in other conditions, it is not specifically elevated in granulosa cell tumors. *Beta-HCG* - **Beta-human chorionic gonadotropin (β-HCG)** is primarily elevated in **gestational trophoblastic disease** (e.g., choriocarcinoma) and some germ cell tumors, such as dysgerminomas and embryonal carcinomas, if they have syncytiotrophoblastic elements [2]. - It is not a typical marker for granulosa cell tumors. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Female Genital Tract, pp. 1036-1037. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Female Genital Tract, pp. 1034-1036.