Biochemical screening of newborn infants by heel-prick blood samples is performed by using the
Q81
Consider the following :
1. Hepatitis A outbreak
2. Polio outbreak
3. Gonorrhoea outbreak through prostitution
Which of the above-listed outbreaks is/are classified under propagated epidemics?
Q82
What is the Body Mass Index of a person 150 cm tall and weighing 67.5 kg?
Q83
Consider the following indices :
1. Chandelier index
2. Sullivan's index
3. Waist-hip index
4. Ponderal index
Which of the above is/are used for measuring obesity?
Q84
Which is the most common cause of mortality in infants between one and twelve months of age in India?
Q85
The cut-off standard for defining low birth-weight babies in India is considered to be
Q86
Sentinel centre for vaccine-preventable diseases does not provide information on
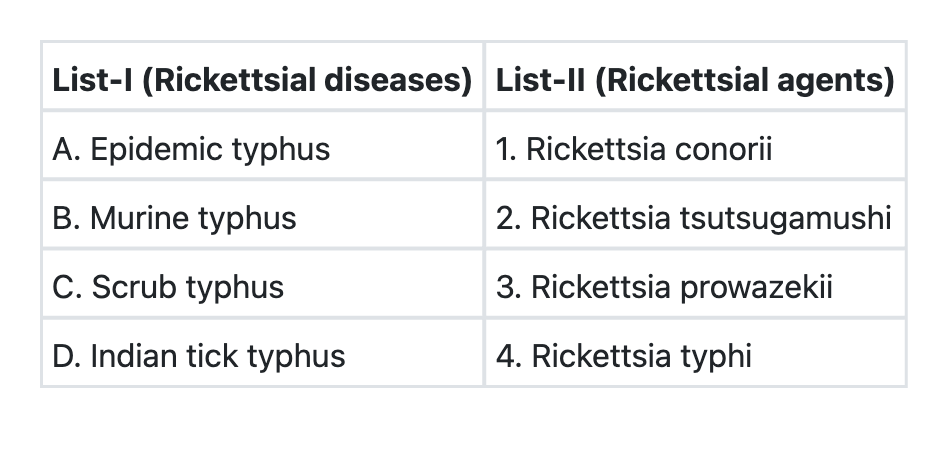
Q81
Match List-I with List-II and select the correct answer using the code given below the Lists:
Q81
Consider the following :
1. Night blindness
2. Corneal xerosis
3. Conjunctival xerosis
4. Keratomalacia
What is the correct sequence of the above in the progress of clinical presentation of vitamin A deficiency blindness?
Q81
With reference to the role of fibre in diet, consider the following statements:
1. It inhibits faecal mutagen synthesis.
2. It reduces post-prandial glucose.
3. It decreases the transit time of food in the bowel.
Which of the above represent(s) the role of fibre in our diet?