All (111)Anatomy (7)Biochemistry (2)Community Medicine (26)ENT (1)Forensic Medicine (1)Internal Medicine (4)Microbiology (6)Obstetrics and Gynecology (27)Ophthalmology (1)Orthopaedics (1)Pathology (9)Pediatrics (3)Pharmacology (5)Physiology (1)Radiology (3)Surgery (14)
Q71
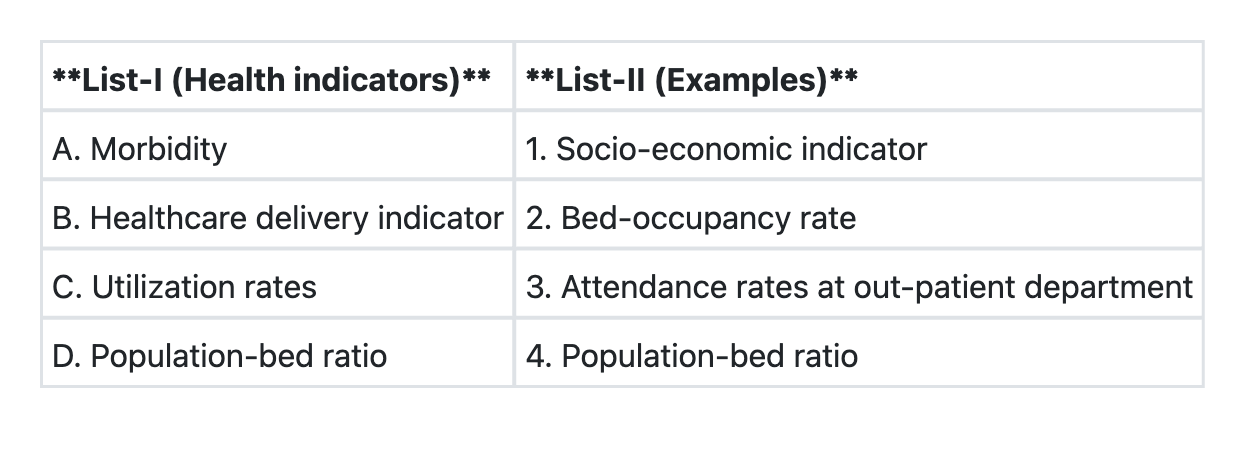
Match List-I with List-II and select the correct answer using the code given below the Lists:
Q72
Winslow's definition of public health does not include which one of the following concepts?
Q73
In a cohort study spanning 20 years, 50 out of 5000 smokers developed lung cancer, and 10 out of 10000 non-smokers developed lung cancer. What is the 'relative risk' among smokers for developing lung cancer?
Q74
A study done in UK of 5174 births at home and 11156 births in hospitals showed perinatal mortality rates of 5.4/1000 in home births and 27.8/1000 in hospital births. What kind of Association is this?
Q75
What is the most cost-effective screening for identifying carcinoma cervix in a population?