All (111)Anatomy (7)Biochemistry (2)Community Medicine (26)ENT (1)Forensic Medicine (1)Internal Medicine (4)Microbiology (6)Obstetrics and Gynecology (27)Ophthalmology (1)Orthopaedics (1)Pathology (9)Pediatrics (3)Pharmacology (5)Physiology (1)Radiology (3)Surgery (14)
Q61
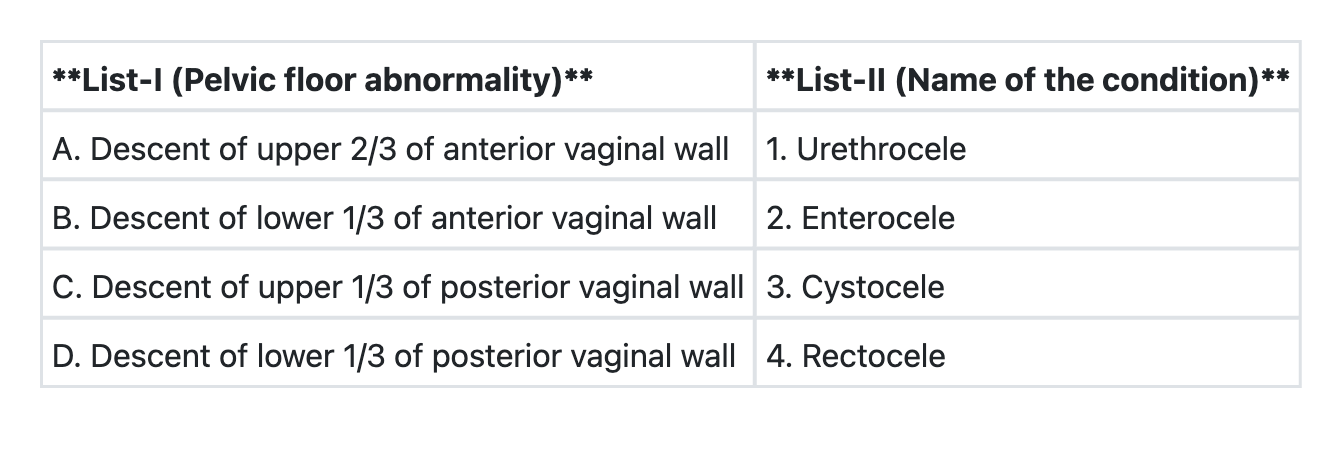
Match List-I with List-II and select the correct answer using the code given below the Lists:
Q62
In a lady with a regular 28-day menstrual cycle, what is the 'safe period'?
Q63
The risk of progression to endometrial cancer from simple hyperplasia without atypia is
Q64
Worldwide, which is the most commonly used copper-bearing intrauterine contraceptive device?
Q65
The following are the contra-indications to the use of combined oral contraceptive pills, except
Q66
Mini pill should be started on the