All (111)Anatomy (7)Biochemistry (2)Community Medicine (26)ENT (1)Forensic Medicine (1)Internal Medicine (4)Microbiology (6)Obstetrics and Gynecology (27)Ophthalmology (1)Orthopaedics (1)Pathology (9)Pediatrics (3)Pharmacology (5)Physiology (1)Radiology (3)Surgery (14)
Q101
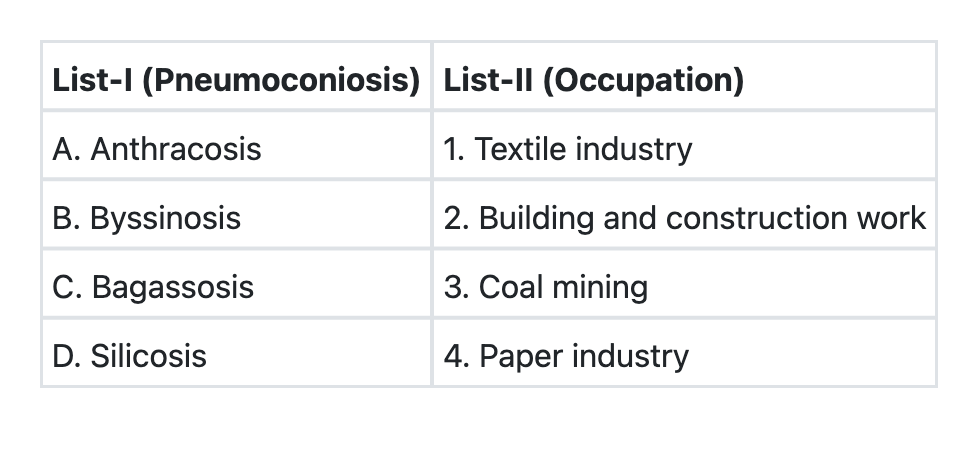
Match List-I with List-II and select the correct answer using the code given below the Lists: List-I (Pneumoconioses): A. Anthracosis B. Byssinosis C. Bagassosis D. Silicosis List-II (Occupational Exposures): 1. Textile industry 2. Coal mining 3. Building and construction work 4. Paper industry Codes:
Q102
In healthcare settings, a series of meetings where individuals work within small groups to arrive at a plan of action for addressing health problems or implementing interventions is called
Q103
Consider the following strategies pertaining to National Anti-Malaria Programme: 1. Early case detection and prompt treatment with ACT (Artemisinin Combination Therapy) 2. Indoor Residual Spraying (IRS) in areas with API ≥2 3. Distribution and promotion of Long Lasting Insecticidal Nets (LLINs) Which of the above strategies is/are being used in India?
Q104
Which is the correct sequence in increasing order for crude birthrates in the countries named herewith?
Q105
Which is the fertility indicator that gives the approximate magnitude of completed family size?
Q106
Consider the following demographic parameters : 1. Average number of daughters born to a woman 2. Sum of age-specific fertility rates 3. Magnitude of completed family size Which of the above parameters reflect/reflects total fertility rate?
Q107
The larvae of which one of the following mosquitoes cannot successfully be killed by spreading oil on the surface of its breeding water sources?