Q11
Abortions in the second trimester mainly occur due to
Q12
Abnormal foetal heart-rate patterns on electronic foetal monitoring include the following, except
Q13
B-Lynch stitch is applied on the uterus for the treatment of
Q14
A 20-year-old nulli-term primigravida is brought to the casualty with labour pains for last 24 hours and a hand prolapse. On examination, she has pulse 96/min, BP 120/80 mm Hg, and mild pallor. The abdominal examination reveals the uterine height at 32 weeks, the foetus in transverse lie and absent foetal heart sounds. On vaginal examination, the left arm of the foetus is prolapsed and the foetal ribs are palpable. The pelvis is adequate. What would be the best management option?
Q15
Regarding the use of a ventouse, which one of the following statements is not correct?
Q16
The presence of a retraction ring at the junction of upper and lower uterine segment in labour indicates
Q17
The indications of an elective caesarean section include all of the following, except
Q18
In the puerperium, which of the following hormonal changes are responsible for lactogenesis? 1. A sudden fall in the oestrogen levels after delivery 2. Reduction of prolactin inhibiting factor from the hypothalamus 3. Release of prolactin from the anterior pituitary 4. Release of oxytocin from the posterior pituitary Select the correct answer using the code given below :
Q19
Match List-I with List-II and select the correct answer using the code given below the Lists:
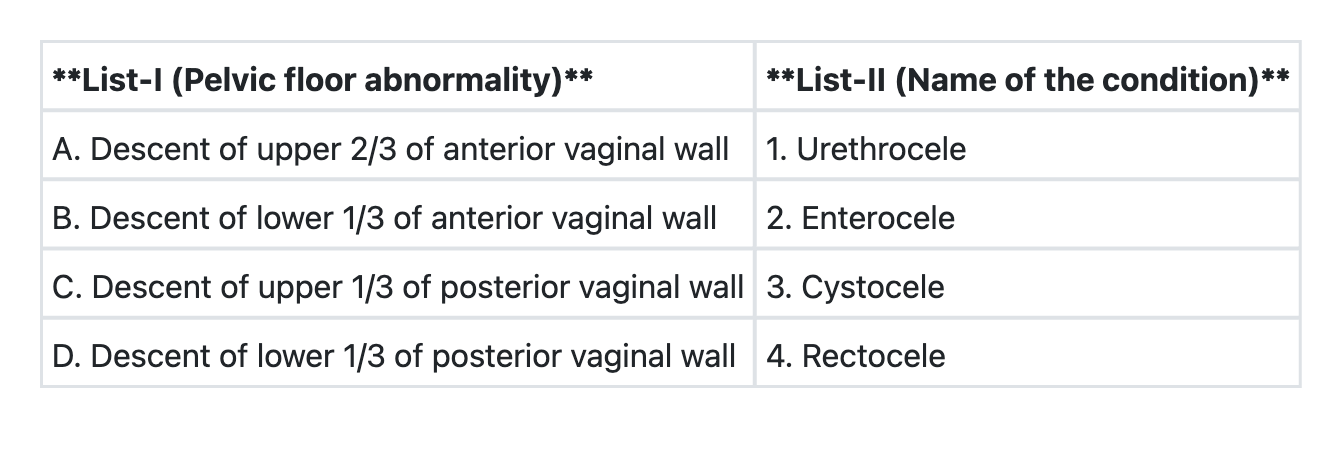
Q20
In a lady with a regular 28-day menstrual cycle, what is the 'safe period'?