UPSC-CMS 2010 — Obstetrics and Gynecology
28 Previous Year Questions with Answers & Explanations
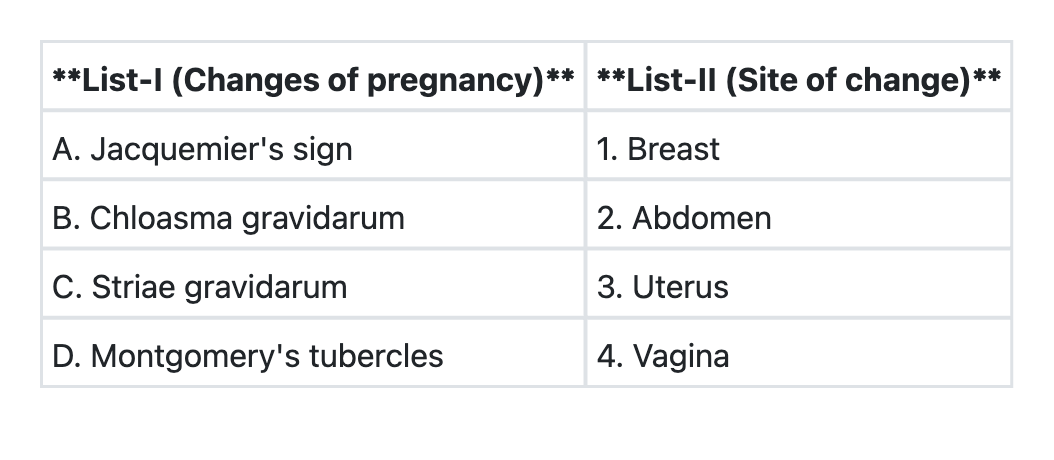
Match List-I (Signs of pregnancy) with List-II (Anatomical sites) and select the correct answer using the code given below the Lists:
If a patient of polycystic ovary syndrome on metformin conceives, how soon should the metformin be stopped?
With reference to the transmission of HIV from mother to child, which one of the following statements is not correct?
Monoamniotic monochorionic twins develop when the division of cell mass occurs
A pregnant woman presents at 28 weeks of gestation with haemoglobin level of 7 gm%; and peripheral smear reveals it to be of microcytic hypochromic type. What would be the correct option of therapy?
Serum AFP (alpha fetoprotein) levels are increased at 16 weeks of pregnancy in all the following conditions, except
The fetal well-being can be assessed by all of the following, except
Match List-I with List-II and select the correct answer using the code given below the Lists:
Which one of the following is diagnosed by Spiegelberg criteria?
Which of the following is the most appropriate management in a ruptured tubal pregnancy?
UPSC-CMS 2010 - Obstetrics and Gynecology UPSC-CMS Practice Questions and MCQs
Question 1: Match List-I (Signs of pregnancy) with List-II (Anatomical sites) and select the correct answer using the code given below the Lists:
- A. A→3 B→4 C→2 D→1 (Correct Answer)
- B. A→3 B→5 C→2 D→1
- C. A→3 B→1 C→4 D→2
- D. A→2 B→4 C→1 D→3
Explanation: ***A→3 B→4 C→2 D→1*** This question has inherent issues as the anatomical sites in List-II do not perfectly correspond to the signs in List-I. Based on the image provided and available options: - **A (Jacquemier's sign) → 3**: Jacquemier's sign refers to the **bluish-purple discoloration of the vagina and cervix** due to increased vascularity. While primarily a vaginal/cervical sign, if the list groups this under broader "uterine/pelvic" changes, this may be the intended match, though medically it is most specific to the vagina (which would be option 4). - **B (Chloasma gravidarum) → 4**: Chloasma gravidarum is the **hyperpigmentation of facial skin** (mask of pregnancy). This does NOT occur on the vagina. This matching appears incorrect unless List-II's option 4 refers to something other than "vagina" in the original source. - **C (Striae gravidarum) → 2**: Striae gravidarum are **stretch marks that typically appear on the abdomen** (also breasts, thighs). This match is **correct**. - **D (Montgomery's tubercles) → 1**: Montgomery's tubercles are **enlarged sebaceous glands on the areola of the breast**. This match is **correct**. *Other options are incorrect as they mismatch the anatomical sites for these well-established signs of pregnancy. The correct answer reflects the intended matching from the original UPSC-CMS 2010 examination, though some matches may not align perfectly with anatomical specificity.*
Question 2: If a patient of polycystic ovary syndrome on metformin conceives, how soon should the metformin be stopped?
- A. Immediately following the diagnosis of pregnancy (Correct Answer)
- B. After the 1st trimester
- C. After the 2nd trimester
- D. Before the onset of labour
Explanation: ***Immediately following the diagnosis of pregnancy*** - Based on **current evidence**, metformin can be safely **discontinued once pregnancy is confirmed** in PCOS patients. - The primary role of metformin in PCOS is to improve **ovulation and achieve conception**—once pregnancy occurs, this goal is accomplished. - Recent large randomized trials (including **PregMet** and **MiTy studies**) have shown **no significant benefit** in continuing metformin during pregnancy for reducing miscarriage or gestational diabetes. - Current practice favors **individualized decisions**, but routine continuation is not standard. *After the 1st trimester* - This was **older practice** based on theoretical benefits of reducing early pregnancy loss. - However, systematic reviews and meta-analyses have **not confirmed** these benefits in well-designed trials. - While some clinicians may continue metformin through the first trimester in selected cases, this is not the standard recommendation for all PCOS pregnancies. *After the 2nd trimester* - Continuing metformin this long is **not evidence-based** for routine PCOS management. - While metformin may be continued throughout pregnancy for **gestational diabetes** management (separate indication), this is not specifically for PCOS. - Most guidelines do not support routine continuation beyond pregnancy confirmation for PCOS alone. *Before the onset of labour* - This timing has **no physiological basis** for PCOS-related metformin use. - If metformin is being used for gestational diabetes (different indication), timing of discontinuation would be individualized, but this is not the standard answer for PCOS patients.
Question 3: With reference to the transmission of HIV from mother to child, which one of the following statements is not correct?
- A. The rate of transmission of HIV from mother to child is between 15-48%
- B. HIV is transmitted through breast milk
- C. In majority of cases, transmission of virus occurs during intrapartum period
- D. Single dose of 200 mg nevirapine at the onset of labour eliminates the risk of HIV transmission to the newborn (Correct Answer)
Explanation: ***Single dose of 200 mg nevirapine at the onset of labour eliminates the risk of HIV transmission to the newborn*** - A single dose of **nevirapine** significantly reduces the risk of mother-to-child transmission (MTCT) but **does not eliminate it completely**. - Elimination of risk would require a comprehensive ART regimen and other preventative measures, which is a significant overstatement. *The rate of transmission of HIV from mother to child is between 15-48%* - The **reported rates** of mother-to-child transmission (MTCT) of HIV, especially in the absence of interventions, generally fall within this range. - This statement is **accurate** regarding the natural history of HIV MTCT without preventative measures. *HIV is transmitted through breast milk* - **Breast milk** is a known route of HIV transmission from mother to child due to the presence of the virus in maternal secretions. - This is why **avoiding breastfeeding** or using antiretroviral prophylaxis is recommended in high-resource settings to prevent transmission. *In majority of cases, transmission of virus occurs during intrapartum period* - The **majority of HIV transmission** from mother to child occurs during **labor and delivery** (intrapartum period) due to exposure to maternal blood and bodily fluids. - A smaller proportion occurs during pregnancy (in utero) or through breastfeeding (postpartum).
Question 4: Monoamniotic monochorionic twins develop when the division of cell mass occurs
- A. after 2 weeks of development of embryonic disc
- B. after 8th day of fertilization (Correct Answer)
- C. within 72 hours after fertilization
- D. between 4th and 8th day of fertilization
Explanation: ***after 8th day of fertilization*** - If division occurs **after the 8th day** post-fertilization, the twins will share both the **amnion** and **chorion**, leading to monoamniotic monochorionic twins. - This late division stage means the **amniotic cavity** has already formed for both embryos, and they share the same amniotic fluid and placenta. *after 2 weeks of development of embryonic disc* - Division this late (after 2 weeks, or day 14) would be extremely rare and usually results in **conjoined twins**, as the embryonic disc has already significantly developed. - At this stage, the primitive streak has formed, and further division would likely involve shared organs or structures. *within 72 hours after fertilization* - Division within the first 72 hours (days 0-3) typically results in **dichorionic diamniotic twins**, meaning each twin has its own placenta and amniotic sac. - This early division occurs before the formation of the inner cell mass and trophoblast differentiate into distinct structures. *between 4th and 8th day of fertilization* - Division between days 4 and 8 most commonly leads to **monochorionic diamniotic twins**, where the twins share a placenta but have separate amniotic sacs. - This timing corresponds to the formation of a common chorion before the development of separate amniotic cavities.
Question 5: A pregnant woman presents at 28 weeks of gestation with haemoglobin level of 7 gm%; and peripheral smear reveals it to be of microcytic hypochromic type. What would be the correct option of therapy?
- A. Blood transfusion
- B. Oral iron and folic acid therapy
- C. Injectable iron therapy (Correct Answer)
- D. Oral iron therapy
Explanation: ***Injectable iron therapy*** - With a hemoglobin of **7 gm%** at **28 weeks of gestation**, the patient has **severe anemia** that requires a rapid increase in hemoglobin. - **Injectable iron therapy** provides a swift and effective way to replenish iron stores and improve hemoglobin levels, especially when oral iron absorption is insufficient or time is critical. *Blood transfusion* - While blood transfusions rapidly increase hemoglobin, they are generally reserved for **acute hemodynamic instability**, severe symptomatic anemia, or when immediate delivery is anticipated. - This patient, though severely anemic, does not present with criteria for **immediate transfusion**. *Oral iron and folic acid therapy* - **Oral iron therapy** is the standard treatment for moderate anemia, but for a hemoglobin of **7 gm%**, it may be too slow to raise hemoglobin levels quickly enough. - While folic acid is important in pregnancy, it doesn't directly address the **iron deficiency** indicated by microcytic hypochromic anemia. *Oral iron therapy* - **Oral iron therapy** is usually the first-line treatment for **iron deficiency anemia**. - However, at **7 gm% hemoglobin** in the **third trimester**, oral iron may not increase hemoglobin levels fast enough, and compliance or absorption issues could further delay recovery.
Question 6: Serum AFP (alpha fetoprotein) levels are increased at 16 weeks of pregnancy in all the following conditions, except
- A. gastroschisis
- B. Down's syndrome (Correct Answer)
- C. multiple pregnancies
- D. neural tube defects
Explanation: ***Down's syndrome*** - This condition is associated with **decreased** levels of maternal serum alpha-fetoprotein (MSAFP), not increased. - Decreased MSAFP, along with elevated human chorionic gonadotropin (hCG) and unconjugated estriol, forms part of the **triple screen** for Down's syndrome. *Gastroschisis* - **Gastroschisis** involves a defect in the abdominal wall allowing fetal intestines to float freely in the amniotic fluid. - This direct exposure of fetal blood vessels in the bowel to amniotic fluid leads to a significant leakage of **AFP**, resulting in markedly elevated maternal serum levels. *Multiple pregnancies* - In **multiple gestations** (e.g., twins or triplets), there are multiple fetuses producing AFP. - The combined production of AFP from all fetuses leads to a proportionally **higher total MSAFP** level, which is a normal finding for such pregnancies. *Neural tube defects* - **Neural tube defects** (NTDs) like anencephaly or spina bifida result from incomplete closure of the neural tube. - This allows **fetal CSF** and neural tissue to leak into the amniotic fluid, leading to significantly elevated levels of AFP in both amniotic fluid and maternal serum.
Question 7: The fetal well-being can be assessed by all of the following, except
- A. non-stress test
- B. ultrasound
- C. contraction stress test
- D. Kleihauer-Betke test (Correct Answer)
Explanation: ***Kleihauer-Betke test*** - The **Kleihauer-Betke test** is used to quantify the amount of **fetal hemoglobin** that has entered the maternal circulation, typically in cases of **fetomaternal hemorrhage**. - It does assess fetal red blood cells in maternal circulation but does not directly assess current fetal well-being in terms of **cardiac activity**, **movement**, or **oxygenation**. *non-stress test* - The **non-stress test (NST)** monitors **fetal heart rate (FHR)** accelerations in response to fetal movement as an indicator of adequate **fetal oxygenation** and **autonomic nervous system function**. - A **reactive NST** with appropriate accelerations is considered a sign of **fetal well-being**. *ultrasound* - **Ultrasound** is a versatile tool for assessing fetal well-being, providing information on **fetal growth**, **anatomy**, **amniotic fluid volume**, and **biophysical profile (BPP)**. - The BPP, which includes ultrasound observations of **fetal breathing**, **movement**, **muscle tone**, and **amniotic fluid volume**, along with an **NST**, offers a comprehensive assessment of fetal status. *contraction stress test* - The **contraction stress test (CST)** evaluates the response of the **fetal heart rate** to uterine contractions, which temporarily reduce placental blood flow. - A **negative CST** (no late decelerations) indicates good **fetal oxygen reserve** and is a reliable sign of **fetal well-being**.
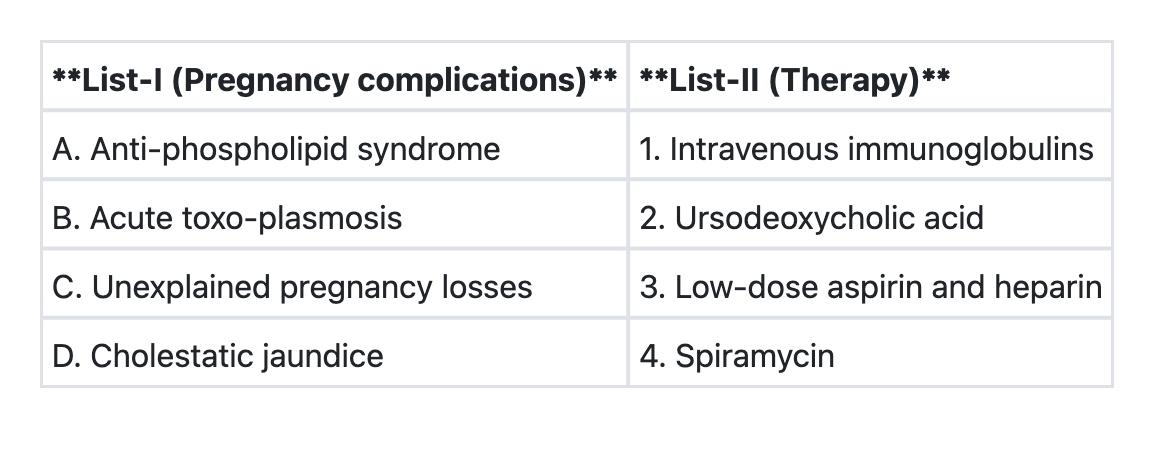
Question 8: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→1 B→4 C→3 D→2
- B. A→2 B→4 C→1 D→3
- C. A→4 B→1 C→3 D→2
- D. A→3 B→4 C→1 D→2 (Correct Answer)
Explanation: ***A→3 B→4 C→1 D→2*** - **Anti-phospholipid syndrome** in pregnancy is managed with **low-dose aspirin and heparin** (usually LMWH) to prevent thrombotic complications and recurrent pregnancy loss. This is the established standard of care supported by multiple clinical trials. - **Acute toxoplasmosis** in pregnancy is treated with **spiramycin** to reduce the risk of vertical transmission to the fetus. Spiramycin concentrates in the placenta without crossing it significantly, thereby limiting parasitic dissemination. If fetal infection is confirmed (after 18 weeks), pyrimethamine plus sulfadiazine is added. - **Unexplained recurrent pregnancy losses** may be managed with **intravenous immunoglobulins (IVIG)** in select cases, particularly when an immunological etiology is suspected. However, the evidence remains controversial and IVIG is not universally recommended as first-line therapy. This answer reflects practices at the time of this examination (2010). - **Cholestatic jaundice** during pregnancy (intrahepatic cholestasis of pregnancy/ICP) is treated with **ursodeoxycholic acid (UDCA)** to improve liver function, reduce maternal serum bile acid levels, and alleviate pruritus. UDCA is the only pharmacological treatment proven to improve biochemical parameters in ICP. *A→1 B→4 C→3 D→2* - This incorrectly associates **Anti-phospholipid syndrome** with IVIG instead of aspirin and heparin, which are the evidence-based treatments for preventing thrombotic complications and pregnancy loss in APS. - Low-dose aspirin and heparin are not indicated for all cases of unexplained pregnancy losses without documented thrombophilia. *A→2 B→4 C→1 D→3* - This incorrectly associates **Anti-phospholipid syndrome** with ursodeoxycholic acid, which is specific for cholestasis of pregnancy, not for thrombophilic conditions. - Aspirin and heparin for **Cholestatic jaundice** would be inappropriate as ICP requires bile acid reduction, not anticoagulation. *A→4 B→1 C→3 D→2* - This incorrectly associates **Anti-phospholipid syndrome** with spiramycin, an antibiotic for toxoplasmosis that has no role in thrombophilia management. - It also incorrectly links **Acute toxoplasmosis** with intravenous immunoglobulins, which have no role in treating this parasitic infection.
Question 9: Which one of the following is diagnosed by Spiegelberg criteria?
- A. Molar pregnancy
- B. Ovarian pregnancy (Correct Answer)
- C. Twin pregnancy
- D. Uterine pregnancy
Explanation: ***Ovarian pregnancy*** - Spiegelberg criteria are specifically used to diagnose an **ovarian ectopic pregnancy**, which is a rare form of ectopic pregnancy where the fertilized egg implants in the ovary. - The criteria include: the **fallopian tube and fimbria are intact** and separate from the ovary, the gestational sac is in the ovarian cortex, it is connected to the uterus by the **ovarian ligament**, and ovarian tissue can be histologically demonstrated in the sac wall. *Molar pregnancy* - This is a type of **gestational trophoblastic disease** characterized by abnormal growth of trophoblastic tissue, resulting in a non-viable pregnancy. - Diagnosis involves high levels of **hCG**, a "snowstorm" appearance on ultrasound, and histopathological examination, not Spiegelberg criteria. *Twin pregnancy* - This refers to the presence of **two fetuses** in a single pregnancy. - Diagnosis is primarily made via **ultrasound imaging** showing two distinct gestational sacs or two fetuses, and is unrelated to Spiegelberg criteria. *Uterine pregnancy* - This is a **normal intrauterine pregnancy** where the fertilized egg implants within the uterine cavity. - It is diagnosed by visualizing a gestational sac and eventually an embryo/fetus within the uterus by **ultrasound**, not by Spiegelberg criteria.
Question 10: Which of the following is the most appropriate management in a ruptured tubal pregnancy?
- A. Autotransfusion of the fresh blood harvested from the peritoneal cavity
- B. Blood transfusion immediately after the clamps have been placed to control the bleeding
- C. Quick resuscitation followed by laparotomy and excision of the offending tube (Correct Answer)
- D. Excision of the offending tube and the ipsilateral ovary (salpingo-oophorectomy)
Explanation: ***Quick resuscitation followed by laparotomy and excision of the offending tube*** - A ruptured tubal pregnancy is a **life-threatening emergency** requiring immediate intervention due to significant hemorrhage. - **Quick resuscitation** (IV fluids, blood products) stabilizes the patient, while **laparotomy** and **excision of the offending tube** are crucial to control bleeding and remove the ectopic pregnancy. *Autotransfusion of the fresh blood harvested from the peritoneal cavity* - While **autotransfusion** can be considered in some trauma cases with large volume internal bleeding, it is not the primary or immediate step in a ruptured ectopic pregnancy. - The immediate priority is to **stop the ongoing bleeding** surgically, as continued hemorrhage outweighs the benefits of autotransfusion if the source is not controlled. *Blood transfusion immediately after the clamps have been placed to control the bleeding* - **Blood transfusion** is essential in managing hemorrhagic shock, but typically begins *during* or *immediately upon presentation* to stabilize the patient, not strictly after surgical clamp placement. - The critical first step is to **achieve hemodynamic stability** (resuscitation) and simultaneously move towards surgical intervention to stop the bleed. *Excision of the offending tube and the ipsilateral ovary (salpingo-oophorectomy)* - **Salpingo-oophorectomy** (removal of tube and ovary) is generally overkill for an ectopic pregnancy, as preserving the ovary is important for future fertility and hormonal function. - A **salpingectomy** (removal of the tube only) is usually sufficient and preferred unless the ovary is also severely damaged or involved.