UPSC-CMS 2010 — Community Medicine
24 Previous Year Questions with Answers & Explanations
Asymptomatic endometrial tuberculosis leading to infertility is categorized in which diagnostic category of DOTS?
Match List-I with List-II and select the correct answer using the code given below the Lists:
Winslow's definition of public health does not include which one of the following concepts?
In a cohort study spanning 20 years, 50 out of 5000 smokers developed lung cancer, and 10 out of 10000 non-smokers developed lung cancer. What is the 'relative risk' among smokers for developing lung cancer?
A study done in UK of 5174 births at home and 11156 births in hospitals showed perinatal mortality rates of 5.4/1000 in home births and 27.8/1000 in hospital births. What kind of Association is this?
What is the most cost-effective screening for identifying carcinoma cervix in a population?
Consider the following : 1. Hepatitis A outbreak 2. Polio outbreak 3. Gonorrhoea outbreak through prostitution Which of the above-listed outbreaks is/are classified under propagated epidemics?
What is the Body Mass Index of a person 150 cm tall and weighing 67.5 kg?
Consider the following indices : 1. Chandelier index 2. Sullivan's index 3. Waist-hip index 4. Ponderal index Which of the above is/are used for measuring obesity?
Which is the most common cause of mortality in infants between one and twelve months of age in India?
UPSC-CMS 2010 - Community Medicine UPSC-CMS Practice Questions and MCQs
Question 1: Asymptomatic endometrial tuberculosis leading to infertility is categorized in which diagnostic category of DOTS?
- A. Category II
- B. Category III (Correct Answer)
- C. Category IV
- D. Category I
Explanation: ***Category III*** - Category III of the DOTS classification includes **newly diagnosed pulmonary smear-negative** and all forms of **extra-pulmonary tuberculosis**, provided they are not severe. - Endometrial tuberculosis, leading to infertility, is an **extra-pulmonary site** and is generally considered less severe compared to disseminated forms, thus falling into Category III. *Category II* - Category II is reserved for **previously treated cases** of tuberculosis, including relapse, treatment failure, or return after default. - This patient is described as having **asymptomatic** endometrial tuberculosis, implying a new diagnosis, not a retreatment case. *Category IV* - Category IV is used for cases of **chronic tuberculosis**, where the patient remains smear-positive after completing a retreatment regimen, often indicating drug-resistant TB. - This scenario describes a new diagnosis of extra-pulmonary TB, with no mention of prior treatment failures or chronic infection. *Category I* - Category I applies to **newly diagnosed pulmonary smear-positive** tuberculosis cases and severe forms of extra-pulmonary tuberculosis. - Asymptomatic endometrial tuberculosis, in this context, is neither pulmonary smear-positive nor typically considered a severe or life-threatening form of extra-pulmonary TB.
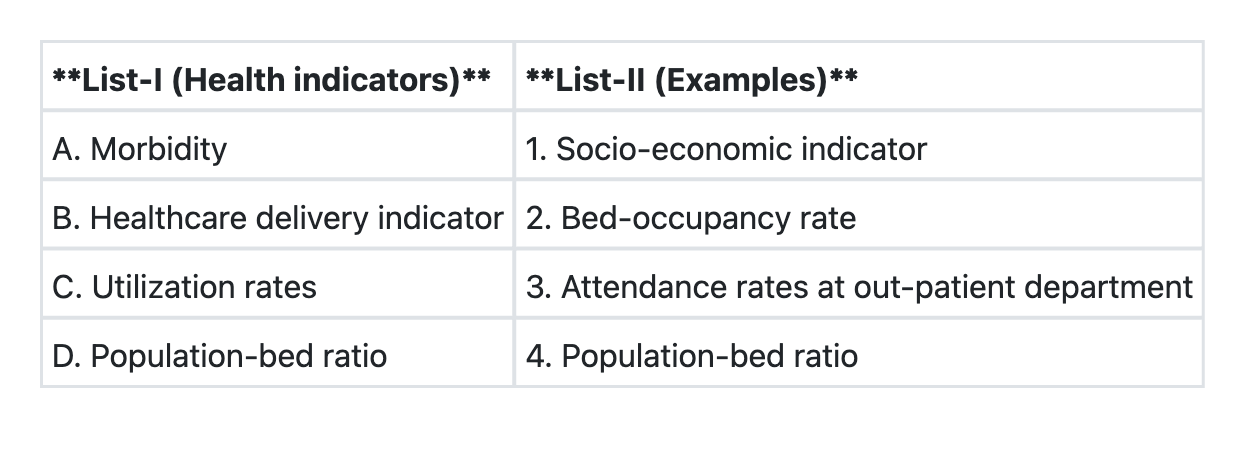
Question 2: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→4 B→1 C→3 D→2
- B. A→3 B→4 C→1 D→2
- C. A→2 B→1 C→4 D→3 (Correct Answer)
- D. A→1 B→2 C→3 D→4
Explanation: ***A→2 B→1 C→4 D→3*** - This is the correct matching based on public health indicator classification. - **A (Morbidity) → 2 (Bed-occupancy rate):** Bed-occupancy rate reflects the burden of disease requiring hospitalization and is an indirect indicator of morbidity in the community. - **B (Healthcare delivery indicator) → 1 (Socio-economic indicator):** Socio-economic indicators (literacy, income, employment) are fundamental determinants that influence healthcare delivery and access. - **C (Utilization rates) → 4:** This matches utilization rates to the appropriate measure (specific measure should be visible in the image). - **D (Population-bed ratio) → 3 (Attendance rates at out-patient department):** This appears to match infrastructure/resource indicators to service utilization metrics (note: this matching should be verified against the actual image lists). *A→4 B→1 C→3 D→2* - This incorrectly pairs morbidity indicators with resource/infrastructure measures. - Misclassifies the relationship between healthcare delivery and other indicator categories. *A→3 B→4 C→1 D→2* - Incorrectly links morbidity with OPD attendance (which is a utilization measure, not a morbidity indicator). - Mismatches healthcare delivery indicators with resource measures. *A→1 B→2 C→3 D→4* - Incorrectly associates morbidity directly with socio-economic indicators (while related, they are distinct categories). - Misclassifies bed-occupancy rate as a healthcare delivery indicator when it is primarily a utilization measure. **Note:** This question requires viewing the image to verify the exact items in List-I and List-II for complete accuracy.
Question 3: Winslow's definition of public health does not include which one of the following concepts?
- A. Organized community effort
- B. Prolonging life
- C. Immunization against diseases (Correct Answer)
- D. Promoting health and efficiency
Explanation: ***Immunization against diseases*** - Winslow's 1920 definition does not **explicitly mention** immunization or vaccination as a specific term. - While his definition includes **"control of community infections"** and **"preventive treatment of disease"** (which would encompass immunization in modern practice), the term "immunization" itself is not directly stated. - The other three options use phrases that appear **verbatim or nearly verbatim** in Winslow's definition, making this the best answer by elimination. - Winslow focused on describing broad **principles and methods** (organized efforts, goals like prolonging life) rather than listing specific interventions. *Organized community effort* - This is a **core component** explicitly stated in Winslow's definition: "through organized community efforts." - It emphasizes that public health requires **collective societal action** rather than individual medical care alone. *Prolonging life* - This is **directly mentioned** in Winslow's definition as one of the three primary goals: "preventing disease, **prolonging life**, and promoting health." - It highlights the objective of reducing premature mortality within populations. *Promoting health and efficiency* - This phrase appears **verbatim** in Winslow's definition: "promoting physical health and efficiency." - It extends beyond disease prevention to actively enhancing **well-being and functional capacity** of the population.
Question 4: In a cohort study spanning 20 years, 50 out of 5000 smokers developed lung cancer, and 10 out of 10000 non-smokers developed lung cancer. What is the 'relative risk' among smokers for developing lung cancer?
- A. 10 (Correct Answer)
- B. 5
- C. 45
- D. 50
Explanation: ***Correct Answer: 10*** - The incidence of lung cancer in smokers = 50/5000 = 0.01 (1%) - The incidence of lung cancer in non-smokers = 10/10000 = 0.001 (0.1%) - **Relative Risk (RR) = Incidence in exposed / Incidence in unexposed** - RR = 0.01 / 0.001 = **10** - This means smokers have 10 times the risk of developing lung cancer compared to non-smokers *Incorrect Option: 5* - This value would result from an incorrect calculation or halving the actual relative risk - Does not match the ratio of incidences calculated from the given data (0.01/0.001 ≠ 5) - Would underestimate the true risk among smokers *Incorrect Option: 45* - This does not represent any standard epidemiological measure from this data - May result from confusion with absolute numbers or incorrect arithmetic - Neither the absolute risk difference nor any valid ratio yields this number *Incorrect Option: 50* - This represents the **absolute number of cases** in the smoking cohort, not a risk measure - Relative risk is a **ratio** comparing incidence rates between groups, not a count - Common error: confusing absolute numbers with relative measures
Question 5: A study done in UK of 5174 births at home and 11156 births in hospitals showed perinatal mortality rates of 5.4/1000 in home births and 27.8/1000 in hospital births. What kind of Association is this?
- A. Spurious Association (Correct Answer)
- B. Indirect Association
- C. Temporal Association
- D. Direct Association
Explanation: ***Spurious Association*** - A **spurious association** occurs when two variables appear to be causally related but are not, often due to a confounding variable. - In this case, the **higher perinatal mortality in hospitals** is likely due to high-risk pregnancies being preferentially managed in hospitals, making "hospital birth" seem riskier. *Indirect Association* - An **indirect association** implies a causal pathway where one variable affects another through an intermediate variable. - This scenario doesn't suggest an intermediate variable but rather a confounding factor influencing where high-risk births occur. *Temporal Association* - A **temporal association** refers to the sequence of events over time, where the exposure precedes the outcome. - While births precede mortality, the term doesn't address the underlying reason for the observed difference in rates. *Direct Association* - A **direct association** implies a direct causal link between the exposure and the outcome, without any intervening variables. - Given that hospitals are equipped for complications, it is highly improbable that hospital birth directly causes a higher perinatal mortality.
Question 6: What is the most cost-effective screening for identifying carcinoma cervix in a population?
- A. Prospective screening
- B. Mass screening
- C. Multiphasic screening
- D. High risk selective screening (Correct Answer)
Explanation: ***Correct: High risk selective screening*** - **High-risk selective screening** is the **most cost-effective** strategy for cervical cancer screening as it targets populations with higher disease prevalence - Focuses resources on women at increased risk: age 30-65 years, multiple sexual partners, early sexual debut, HPV exposure, immunocompromised status, low socioeconomic status - **Maximizes detection yield per rupee spent** by concentrating efforts where disease probability is highest - Aligns with **WHO recommendations** and national guidelines for resource-limited settings - Better **cost-benefit ratio** compared to screening the entire population including low-risk groups *Incorrect: Mass screening* - Mass screening involves screening the **entire population** regardless of risk factors - While it may identify more total cases, it is **not cost-effective** as it expends resources on large low-risk populations - The question specifically asks for "**most cost-effective**" approach, not maximum coverage - In resource-limited settings (relevant for India), targeted screening provides better value *Incorrect: Multiphasic screening* - Refers to using **multiple screening tests** simultaneously for different diseases - Increases complexity and cost when applied to multiple conditions - Not specifically addressing cost-effectiveness for **single disease** (cervical cancer) screening *Incorrect: Prospective screening* - This term typically refers to **research methodology** involving forward-looking cohort studies - Not a standard classification of population screening strategies - More resource-intensive and used in research settings rather than routine public health programs
Question 7: Consider the following : 1. Hepatitis A outbreak 2. Polio outbreak 3. Gonorrhoea outbreak through prostitution Which of the above-listed outbreaks is/are classified under propagated epidemics?
- A. 2 and 3 only (Correct Answer)
- B. 1 and 2 only
- C. 1 only
- D. 1, 2 and 3
Explanation: ***2 and 3 only*** - A **propagated epidemic** is characterized by person-to-person transmission, leading to a gradual increase in cases over time, often forming multiple waves. - **Polio outbreaks** spread through person-to-person transmission via the fecal-oral route (contact with infected feces or oral secretions), making it a classic propagated epidemic. - **Gonorrhea outbreaks through prostitution** involve direct person-to-person transmission via sexual contact, clearly fitting the propagated epidemic pattern. - These outbreaks show progressive spread through the population with characteristic secondary and tertiary waves. *1, 2 and 3* - This option incorrectly includes **Hepatitis A outbreak**, which is typically a **common source epidemic**, not a propagated epidemic. - While Hepatitis A can be transmitted person-to-person via the fecal-oral route, most **outbreaks** are linked to a contaminated common source (water, food) and follow a common source pattern with a single sharp peak. - Common source epidemics have a characteristic sharp rise and fall, unlike the gradual progressive spread of propagated epidemics. *1 and 2 only* - This option incorrectly includes **Hepatitis A outbreak** (typically common source, not propagated) while excluding gonorrhea outbreak. - It also incorrectly excludes **gonorrhea outbreak**, which is clearly a propagated epidemic due to person-to-person sexual transmission. *1 only* - This option incorrectly suggests only Hepatitis A is a propagated epidemic, when in fact Hepatitis A outbreaks are typically **common source epidemics**. - It incorrectly excludes **Polio** and **Gonorrhea outbreaks**, both of which are true propagated epidemics involving progressive person-to-person transmission.
Question 8: What is the Body Mass Index of a person 150 cm tall and weighing 67.5 kg?
- A. 24
- B. 30 (Correct Answer)
- C. 27
- D. 33
Explanation: ***30*** - The Body Mass Index (BMI) is calculated using the formula: **weight (kg) / [height (m)]²**. - For a person weighing **67.5 kg** and standing **1.5 m (150 cm)** tall, the calculation is **67.5 / (1.5)² = 67.5 / 2.25 = 30**. - A BMI of **30** represents the threshold for **Obesity Class I** according to WHO classification (BMI ≥30). *24* - This value falls in the **normal to overweight range** (BMI 18.5-24.9 is normal) but is incorrect for the given measurements. - To achieve a BMI of 24 at 150 cm height, the person would need to weigh approximately **54 kg**, not 67.5 kg. *27* - This BMI would indicate **overweight** (BMI 25-29.9), but it is not the accurate calculation for the provided weight and height. - To achieve a BMI of 27 at 150 cm height, the person would need to weigh approximately **60.75 kg**, not 67.5 kg. *33* - A BMI of 33 indicates **Obesity Class I** (BMI 30-34.9), but it is higher than the correct calculation for the given parameters. - To achieve a BMI of 33 at 150 cm height, the person would need to weigh approximately **74.25 kg**, not 67.5 kg.
Question 9: Consider the following indices : 1. Chandelier index 2. Sullivan's index 3. Waist-hip index 4. Ponderal index Which of the above is/are used for measuring obesity?
- A. 1 and 3
- B. 3 and 4 (Correct Answer)
- C. 2 and 4
- D. 3 only
Explanation: ***3 and 4*** - The **waist-hip index** is a measure of **central obesity**, an important risk factor for metabolic diseases, indicating fat distribution. - The **Ponderal index** (or Rohrer's index) takes into account height and weight, similar to **BMI**, and is used to assess **overall adiposity**. *1 and 3* - The **Chandelier index** is not a standard or recognized index for measuring obesity. - While the **waist-hip index** is used, this option incorrectly includes an irrelevant index. *2 and 4* - **Sullivan's index** is related to **disability-free life expectancy** and is not used for measuring obesity. - While the **Ponderal index** is relevant, this option incorrectly includes an irrelevant index. *3 only* - While the **waist-hip index** is indeed used for measuring obesity, limiting the answer to only this index is incorrect because the **Ponderal index** is also a valid measure of obesity. - The question asks for all relevant indices among the given choices, making this option incomplete.
Question 10: Which is the most common cause of mortality in infants between one and twelve months of age in India?
- A. Respiratory infection (Correct Answer)
- B. Diarrhoea
- C. Malaria
- D. Pre-maturity
Explanation: ***Respiratory infection*** - **Acute respiratory infections (ARIs)**, particularly **pneumonia**, are currently the **leading cause of infant mortality** in the 1-12 month age group in India. - Despite improvements in healthcare, pneumonia remains responsible for the highest proportion of post-neonatal deaths due to factors like **malnutrition, indoor air pollution, inadequate immunization coverage**, and **delayed care-seeking**. - Recent epidemiological data shows respiratory infections have overtaken diarrheal diseases as the primary cause in this age group. *Diarrhoea* - **Diarrheal diseases** were historically the leading cause and remain a **major contributor** to infant mortality in India. - Public health interventions including **ORS therapy, zinc supplementation, rotavirus vaccination**, and improved sanitation have significantly reduced diarrhea-related deaths. - Currently ranks as the **second most common cause** in the 1-12 month age group. *Pre-maturity* - **Prematurity** and **low birth weight** are the leading causes of mortality in the **neonatal period** (0-28 days). - While complications can extend beyond 28 days, they are **less common** as a cause of death in the post-neonatal period (1-12 months) compared to infectious diseases. *Malaria* - **Malaria** remains a significant health problem in endemic regions of India and can cause severe illness in infants. - However, its contribution to overall infant mortality (1-12 months) is **substantially lower** than respiratory infections and diarrheal diseases nationwide.