UPSC-CMS 2010
111 Previous Year Questions with Answers & Explanations
Biochemistry
1 questionsWhich one of the following biochemical abnormalities can be produced by repeated vomiting?
UPSC-CMS 2010 - Biochemistry UPSC-CMS Practice Questions and MCQs
Question 1: Which one of the following biochemical abnormalities can be produced by repeated vomiting?
- A. Metabolic acidosis
- B. Metabolic alkalosis (Correct Answer)
- C. Ketosis
- D. Uraemia
Explanation: ***Metabolic alkalosis*** - Repeated vomiting leads to the loss of **hydrochloric acid (HCl)** from the stomach, causing **hypochloremic metabolic alkalosis** with an increase in serum **bicarbonate (HCO3-)** and a rise in blood pH. - The loss of H+ and Cl- ions results in **compensatory hypokalemia** as the kidneys exchange K+ for H+ to maintain electroneutrality. - **Volume depletion** from vomiting triggers aldosterone secretion, which further promotes K+ loss and H+ excretion, perpetuating the alkalosis (contraction alkalosis). - This is one of the most common causes of metabolic alkalosis in clinical practice. *Metabolic acidosis* - This condition is characterized by a decrease in **serum pH** and **bicarbonate levels**, typically due to excess acid production or bicarbonate loss from diarrhea or renal tubular acidosis. - Vomiting does not directly cause metabolic acidosis; rather, it leads to the opposite effect by removing acidic gastric contents. *Ketosis* - **Ketosis** occurs when the body metabolizes fat for energy, producing **ketone bodies**, common in conditions like uncontrolled diabetes or prolonged starvation. - While severe, prolonged vomiting with reduced oral intake can indirectly lead to starvation ketosis, the primary and most characteristic biochemical abnormality of repeated vomiting is metabolic alkalosis, not ketosis. *Uraemia* - **Uraemia** is a syndrome caused by the accumulation of **nitrogenous waste products** (urea, creatinine) in the blood, primarily due to kidney failure. - Vomiting may be a *symptom* of uraemia, but it does not *cause* uraemia. Kidney function is the primary determinant of urea levels.
Internal Medicine
2 questionsA patient presents with claudication in both buttocks and has impotence. The clinical examination reveals bruit over lower abdomen. What is the clinical diagnosis?
The normal ankle brachial pressure index (ABPI) is 1.0. A value of 0.8 suggests
UPSC-CMS 2010 - Internal Medicine UPSC-CMS Practice Questions and MCQs
Question 1: A patient presents with claudication in both buttocks and has impotence. The clinical examination reveals bruit over lower abdomen. What is the clinical diagnosis?
- A. Bilateral iliofemoral occlusion
- B. Aortoiliac occlusion (Correct Answer)
- C. Bilateral iliac artery occlusion
- D. Bilateral femoropopliteal occlusion
Explanation: Aortoiliac occlusion - The triad of **buttock claudication**, **impotence**, and **absent or diminished femoral pulses** (often associated with an abdominal bruit) is classic for **Leriche syndrome**, which is caused by aortoiliac occlusion [2], [3]. - This occlusion impairs blood flow to both lower extremities and the internal iliac arteries, affecting erectile function [1]. Bilateral iliofemoral occlusion - While this would cause bilateral lower limb symptoms, it typically would not explain the **impotence** as clearly as an aortoiliac occlusion which affects the internal iliac arteries that supply the penis [2], [3]. - An iliofemoral occlusion is distal to the aorta, and the symptom complex provided points to a more **proximal lesion**. Bilateral iliac artery occlusion - This would cause similar symptoms to aortoiliac occlusion including **buttock claudication** and **impotence** [2]. - However, the presence of a **bruit over the lower abdomen** often indicates a more proximal lesion involving the aorta, making aortoiliac occlusion a more comprehensive diagnosis for these findings. Bilateral femoropopliteal occlusion - This would primarily cause **calf and thigh claudication**, less commonly buttock claudication, as the occlusion is more distal [1]. - **Impotence** is not a typical symptom of isolated femoropopliteal occlusion, as the internal iliac arteries are usually unaffected.
Question 2: The normal ankle brachial pressure index (ABPI) is 1.0. A value of 0.8 suggests
- A. impending gangrene
- B. presence of collaterals
- C. some degree of arterial obstruction (Correct Answer)
- D. good flow
Explanation: ***some degree of arterial obstruction*** - An **ABPI of 0.8** indicates a reduction in blood flow to the lower extremities compared to the upper limbs [1]. - This value is generally considered to signify **mild to moderate peripheral artery disease (PAD)**, suggesting the presence of arterial narrowing or obstruction [1]. *impending gangrene* - **Impending gangrene** or critical limb ischemia is typically associated with a much lower ABPI, usually **below 0.4** or even 0.3 [1]. - At an ABPI of 0.8, severe tissue damage and gangrene are not imminent, although careful monitoring is still warranted. *presence of collaterals* - While **collateral arteries** can develop in response to chronic arterial obstruction, an ABPI of 0.8 primarily reflects the overall net blood flow, which is still reduced despite collaterals [1]. - The presence of collaterals can actually help to maintain tissue viability and prevent more severe symptoms, but they don't normalize the ABPI in the presence of significant disease [1]. *good flow* - A value of **1.0 to 1.4** is generally considered a normal ABPI, indicating good arterial flow. - An ABPI of **0.8 is significantly below normal** and suggests impaired rather than good blood flow [1].
Microbiology
1 questionsAutoclaving is a method of sterilization. The process involves heating by steam at
UPSC-CMS 2010 - Microbiology UPSC-CMS Practice Questions and MCQs
Question 1: Autoclaving is a method of sterilization. The process involves heating by steam at
- A. 10 lb pressure, 100 °C temperature for 10 minutes
- B. 20 lb pressure, 120 °C temperature for 20 minutes
- C. 15 lb pressure, 121 °C temperature for 15 minutes (Correct Answer)
- D. 25 lb pressure, 120 °C temperature for 25 minutes
Explanation: ***15 lb pressure, 121 °C temperature for 15 minutes*** - This is the **standard recommended parameter** for routine sterilization in an autoclave, ensuring the destruction of most pathogenic and non-pathogenic microorganisms, including spores. - The combination of **steam at 121°C** (equivalent to 15 psi) for at least 15 minutes provides efficient heat transfer and penetration required for effective sterilization. *10 lb pressure, 100 °C temperature for 10 minutes* - This temperature (100 °C) is used for **boiling** or pasteurization, which is generally not sufficient for complete sterilization as it may not kill highly resistant spores. - The **lower pressure and temperature** would likely not achieve the required sterility assurance level. *20 lb pressure, 120 °C temperature for 20 minutes* - While higher pressure can achieve sterilization, this is **not the standard parameter** used for typical autoclave sterilization. - The standard combination of 15 lb at 121°C is more commonly recommended and taught in medical curricula. *25 lb pressure, 120 °C temperature for 25 minutes* - This combination of **higher pressure and longer duration** would likely achieve sterilization, but it exceeds the minimum standard parameters. - While effective, it is not the most **efficient or commonly recommended** setting and could potentially lead to material degradation for some items.
Pathology
2 questionsHypertrophic scar is characterized by the following, except
Langhans' giant cells are characteristically seen in
UPSC-CMS 2010 - Pathology UPSC-CMS Practice Questions and MCQs
Question 1: Hypertrophic scar is characterized by the following, except
- A. it involves the flexor surface
- B. it outgrows the wound area (Correct Answer)
- C. it is non-familial
- D. it is not related to the race
Explanation: ***it outgrows the wound area*** - This statement is characteristic of a **keloid scar**, not a hypertrophic scar. Keloids are distinguished by their growth beyond the original wound margins [1]. - **Hypertrophic scars**, on the other hand, remain confined within the boundaries of the original injury, though they may be raised and erythematous [1]. *it involves the flexor surface* - While hypertrophic scars can occur on any body surface, they are commonly found on areas of **high tension**, such as the **flexor surfaces** of joints (e.g., knee, elbow) or the chest and shoulders. - This involvement is due to constant movement stretching the healing skin, which can stimulate excessive collagen production. *it is non-familial* - Hypertrophic scars are generally **not associated with a strong genetic predisposition** or familial inheritance patterns. - Their development is primarily linked to factors like wound tension, infection, and individual healing responses rather than inherited tendencies. *it is not related to the race* - The incidence of hypertrophic scars does **not show a significant racial predilection**, unlike keloid scars, which are more common in individuals with darker skin types. - Hypertrophic scars can affect individuals from all racial backgrounds. **References:** [1] Kumar v, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Inflammation and Repair, pp. 119-121.
Question 2: Langhans' giant cells are characteristically seen in
- A. typhoid Peyer's patch
- B. peritoneal tuberculosis (Correct Answer)
- C. tuberculoma
- D. lymphoma
Explanation: ***Peritoneal tuberculosis*** - **Langhans' giant cells** are a characteristic histological feature of **granulomatous inflammation**, particularly seen in **tuberculosis** [1], [2]. - They are formed by the fusion of epithelioid histiocytes and are a hallmark of **mycobacterial infections**, including peritoneal tuberculosis [2]. - While not pathognomonic, their presence in the appropriate clinical context strongly suggests tuberculosis [1]. *Typhoid Peyer's patch* - **Typhoid fever** causes **macrophage infiltration** with **necrosis** and **ulceration** in Peyer's patches. - The inflammatory response is mononuclear but does **not** form **epithelioid granulomas** or Langhans' giant cells. - Histology shows mononuclear cell infiltration and typhoid nodules, not granulomatous inflammation. *Tuberculoma* - A **tuberculoma** is a localized form of tuberculosis and **also contains Langhans' giant cells** within its granulomatous structure [1]. - However, peritoneal tuberculosis represents a broader clinical entity where identification of these cells in peritoneal tissue/fluid is diagnostically significant. - Both are forms of TB, but the question context favors the systemic/cavity involvement over a localized mass lesion. *Lymphoma* - **Lymphoma** shows malignant proliferation of lymphoid cells with effacement of normal architecture. - It does **not** show **granulomatous inflammation** or Langhans' giant cells. - Histology reveals sheets of atypical lymphoid cells, not epithelioid granulomas. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Infectious Diseases, pp. 383-384. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Inflammation and Repair, p. 109.
Pharmacology
1 questionsMatch List-I with List-II and select the correct answer using the code given below the Lists:
UPSC-CMS 2010 - Pharmacology UPSC-CMS Practice Questions and MCQs
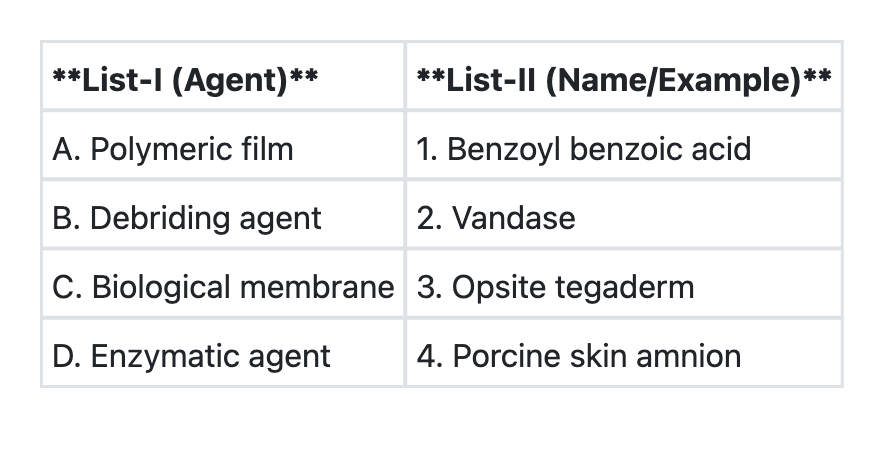
Question 1: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→3 B→1 C→2 D→4
- B. A→1 B→2 C→4 D→3
- C. A→3 B→2 C→4 D→1 (Correct Answer)
- D. A→1 B→2 C→3 D→4
Explanation: ***A→1 B→2 C→3 D→4*** - This represents the **best available matching** among the given options, where each category is paired with the most appropriate example from the choices provided. - While not the ideal pharmacological classification, this option provides the most logical **wound care agent pairing** within the constraints of the available answers. *A→3 B→1 C→4 D→2* - Incorrectly matches **debriding agent (B)** with **benzoyl benzoic acid (1)**, which is primarily a **keratolytic agent** rather than a debriding agent. - Misplaces **enzymatic agent (D)** with **Vandase (2)**, when Vandase is better classified as a **debriding enzyme**. *A→3 B→1 C→2 D→4* - Incorrectly pairs **biological membrane (C)** with **Vandase (2)**, which is an **enzymatic preparation** not a biological membrane. - Creates multiple **mismatched classifications** that don't align with standard wound care categories. *A→1 B→2 C→4 D→3* - Incorrectly matches **polymeric film (A)** with **benzoyl benzoic acid (1)**, which is not a **film dressing** but a topical agent. - Misplaces **enzymatic agent (D)** with **Opsite/Tegaderm (3)**, which are **synthetic polymeric films** not enzymatic preparations.
Surgery
3 questionsIn carcinoma breast, adjuvant radiotherapy is indicated after modified radical mastectomy in all of the following, except
The percutaneous PAIR therapy used in the treatment of uncomplicated hepatic hydatid cyst can be associated with the following complications, except
Trendelenburg's operation is done for
UPSC-CMS 2010 - Surgery UPSC-CMS Practice Questions and MCQs
Question 1: In carcinoma breast, adjuvant radiotherapy is indicated after modified radical mastectomy in all of the following, except
- A. more than four positive axillary lymph nodes
- B. positive margins
- C. tumour size more than 5 cm
- D. ER, PR hormone receptor negative tumour (Correct Answer)
Explanation: ***ER, PR hormone receptor negative tumour*** - While **ER/PR negative** tumors (including triple-negative breast cancers) are often more aggressive and have higher recurrence rates, **adjuvant radiotherapy** post-mastectomy is primarily dictated by **local-regional anatomic and pathologic factors**, not solely by receptor status. - **ER/PR negative status is NOT a standalone indication** for post-mastectomy radiation therapy (PMRT) in guidelines. The decision for radiotherapy is based on **tumor burden, nodal involvement, and surgical margins**. - Receptor status influences systemic therapy choices but does not independently determine the need for radiotherapy after adequate surgical resection. *more than four positive axillary lymph nodes* - The presence of **four or more positive axillary lymph nodes** is one of the **strongest indications** for post-mastectomy radiation therapy. - This degree of nodal involvement significantly increases the risk of locoregional recurrence, and **PMRT is standard of care** in this scenario. - Guidelines consistently recommend radiotherapy to the chest wall and regional nodal basins when ≥4 nodes are positive. *positive margins* - **Positive surgical margins** after mastectomy indicate residual tumor cells along the resection edges, representing an **absolute indication** for adjuvant radiotherapy if re-excision is not feasible. - This is a **pathologic criterion** that directly indicates microscopic residual disease requiring radiation for local control. - PMRT significantly reduces local recurrence risk in this high-risk scenario. *tumour size more than 5 cm* - A **tumor size greater than 5 cm** (T3 classification) is an **established indication** for post-mastectomy radiation therapy, independent of nodal status. - This substantial tumor burden is associated with higher locoregional recurrence risk even after complete surgical resection. - **PMRT improves locoregional control** and overall outcomes in patients with T3 tumors.
Question 2: The percutaneous PAIR therapy used in the treatment of uncomplicated hepatic hydatid cyst can be associated with the following complications, except
- A. hypotension
- B. bradycardia (Correct Answer)
- C. vomiting
- D. anaphylaxis
Explanation: ***bradycardia*** - **Bradycardia is not a recognized primary complication** of percutaneous aspiration, injection, and re-aspiration (PAIR) therapy for hydatid cysts. - While bradycardia can occur as a **vasovagal response during any invasive procedure**, it is not specifically listed among the complications of PAIR therapy in standard medical literature. - The typical cardiovascular manifestation of anaphylaxis (a known PAIR complication) is **tachycardia**, not bradycardia. *hypotension* - **Hypotension** is a well-documented complication of PAIR therapy, occurring due to **anaphylactic reaction** from leakage of antigenic hydatid fluid into the circulation. - It can also result from **intra-abdominal hemorrhage** if a major vessel is inadvertently punctured during the procedure. *vomiting* - **Vomiting** can occur as part of a **systemic allergic reaction or anaphylaxis** triggered by the release of hydatid cyst contents. - It may also be a manifestation of peritoneal irritation if cyst contents leak into the peritoneal cavity. *anaphylaxis* - **Anaphylaxis** is the most feared and well-documented complication of PAIR therapy, caused by the release of **highly antigenic hydatid cyst fluid** (containing protoscolices and hydatid antigens) into the host's system. - This severe Type I hypersensitivity reaction can manifest with **hypotension, tachycardia, bronchospasm, urticaria, angioedema**, and in severe cases, cardiovascular collapse. - Prophylactic antihistamines and corticosteroids are often administered to minimize this risk.
Question 3: Trendelenburg's operation is done for
- A. primary varicose veins (Correct Answer)
- B. deep vein thrombosis with varicose veins
- C. varicocele
- D. arteriovenous fistula
Explanation: ***primary varicose veins*** - **Trendelenburg's operation** is the classical surgical procedure for **primary varicose veins of the lower limb** - It involves **high ligation of the long saphenous vein** at the saphenofemoral junction - Named after Friedrich Trendelenburg (1844-1924), this was historically the standard treatment for varicose veins - Modern variations include **flush ligation** and stripping of the saphenous vein - Now often replaced by minimally invasive techniques like **endovenous laser ablation (EVLA)** and **radiofrequency ablation (RFA)** *varicocele* - **Varicocele** is treated by operations like **Ivanissevich procedure**, **Palomo's operation**, or **laparoscopic varicocelectomy** - These involve ligation of the **testicular/gonadal veins**, not the saphenous vein - There is no established surgical technique for varicocele called "Trendelenburg's operation" - The confusion may arise from Trendelenburg's contributions to various surgical fields *deep vein thrombosis with varicose veins* - **Deep vein thrombosis (DVT)** is an acute condition requiring **anticoagulation therapy**, not surgical intervention like Trendelenburg's operation - Management focuses on preventing **pulmonary embolism** and post-thrombotic syndrome - Varicose veins may coexist but are addressed separately after DVT treatment *arteriovenous fistula* - **Arteriovenous fistula** represents an abnormal connection between artery and vein - Treatment involves **surgical repair**, **embolization**, or observation depending on etiology - This is unrelated to Trendelenburg's operation for venous insufficiency
About UPSC-CMS 2010 Questions
This page contains 111 questions from the UPSC-CMS 2010 paper, organised across 16 subjects for focused practice. Every question comes with the correct answer and a detailed explanation to help you understand the underlying concept. Subject-wise organisation lets you target specific areas and identify which topics carried the most weight in this particular year.
Practising year-wise papers is essential for understanding how the UPSC-CMS exam evolves — you can spot trending topics, gauge difficulty shifts, and benchmark your readiness against a real paper. To take your preparation further, download the Oncourse app for AI-driven performance insights, spaced repetition of questions you got wrong, and a personalised study plan built around your UPSC-CMS goals.