All (107)Anatomy (3)Anesthesiology (1)Biochemistry (4)Community Medicine (27)Dermatology (1)Forensic Medicine (1)Internal Medicine (8)Microbiology (4)Obstetrics and Gynecology (26)Pathology (4)Pediatrics (2)Pharmacology (4)Physiology (2)Radiology (1)Surgery (19)
Q31
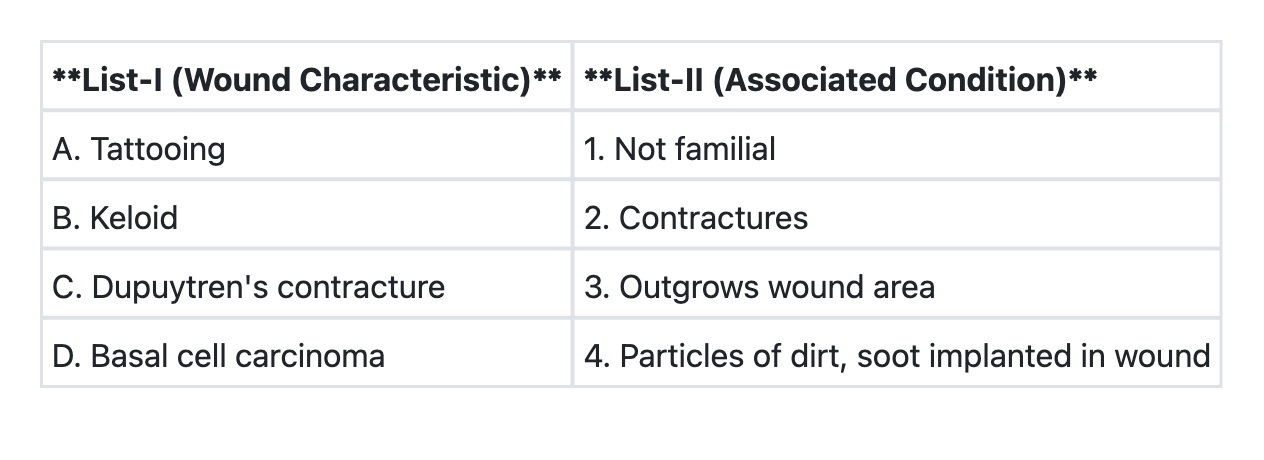
Match List-I with List-II and select the correct answer using the code given below the Lists: (Refer to the image for List-I and List-II)
Q32
Which of the following is the best indicator of prognosis of soft tissue sarcoma?
Q33
Lympho-venous anastomosis is done for
Q34
Which one of the following investigations is considered to be "Gold standard" technique for diagnosis of arterial occlusive disease ?
Q35
Which one of the following statements is not correct regarding thoracic outlet syndrome?