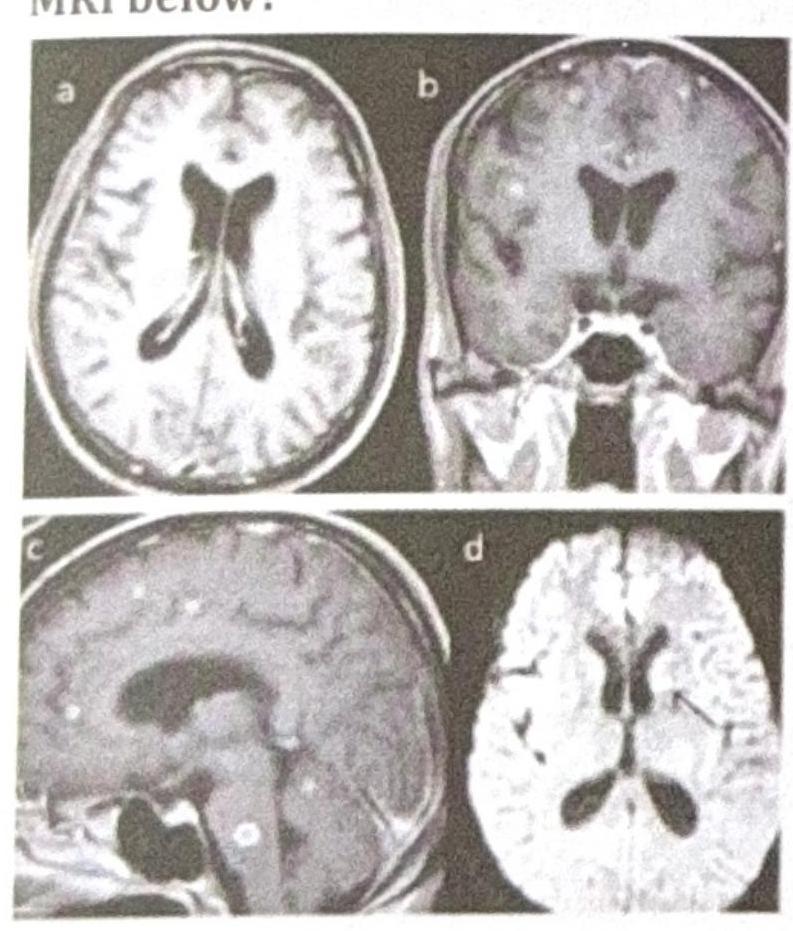
A patient presents with seizures that were controlled with midazolam. Lumbar puncture (LP) revealed no pathology. What is the confirmatory test in the condition shown in the MRI below?
NEET-PG 2024 - Internal Medicine NEET-PG Practice Questions and MCQs
Question 1: A patient presents with seizures that were controlled with midazolam. Lumbar puncture (LP) revealed no pathology. What is the confirmatory test in the condition shown in the MRI below?
A. PET scan
B. CBNAAT
C. MR spectroscopy (Correct Answer)
D. MRI serial scan
Explanation: ***MR spectroscopy***
- The MRI shows multiple **ring-enhancing lesions**, which, combined with the history of seizures and normal LP, strongly suggests **neurocysticercosis**.
- **MR spectroscopy** can detect the specific biochemical markers (e.g., lactate, succinate) within the cyst, which are indicative of the parasitic infection, and can help differentiate it from other lesions like tumors or abscesses.
*PET scan*
- A **PET scan** primarily assesses metabolic activity and is more commonly used in the evaluation of tumors or neurodegenerative diseases.
- It is generally not the primary or confirmatory test for neurocysticercosis, as it does not directly visualize the parasite or its specific biochemical markers.
*CBNAAT*
- **CBNAAT (Cartridge-Based Nucleic Acid Amplification Test)** is a rapid molecular test primarily used for the diagnosis of **tuberculosis**, not neurocysticercosis.
- While tuberculosis can cause CNS lesions, the clinical and imaging presentation (multiple ring-enhancing lesions) is more suggestive of neurocysticercosis, and CBNAAT would not confirm this diagnosis.
*MRI serial scan*
- **Serial MRI scans** are useful for monitoring the progression or resolution of lesions over time, especially in response to treatment.
- However, a serial scan is not a "confirmatory test" for the initial diagnosis; it provides prognostic or follow-up information rather than confirming the etiology.
OB/GYN
1 questions
Q1
A 30-year-old woman presents with a history of pelvic pain and infertility. A transvaginal ultrasound is performed, and the image provided shows a tubular, fluid-filled structure with thin walls. There is no evidence of solid components or internal septations. What is the most likely diagnosis?
NEET-PG 2024 - OB/GYN NEET-PG Practice Questions and MCQs
Question 1: A 30-year-old woman presents with a history of pelvic pain and infertility. A transvaginal ultrasound is performed, and the image provided shows a tubular, fluid-filled structure with thin walls. There is no evidence of solid components or internal septations. What is the most likely diagnosis?
A. Ovarian cyst
B. Ectopic pregnancy
C. Hydrosalpinx (Correct Answer)
D. Endometrioma
E. Tubo-ovarian abscess
Explanation: ***Hydrosalpinx***
- The ultrasound finding of a **tubular, fluid-filled structure with thin walls** and no solid components or septations is highly characteristic of a **hydrosalpinx**, which is a blocked, fluid-filled fallopian tube.
- **Pelvic pain** and **infertility** in a young woman are classic clinical presentations associated with hydrosalpinx, often resulting from previous pelvic inflammatory disease.
*Ovarian cyst*
- While ovarian cysts are fluid-filled, they typically appear as **rounded or oval structures within or adjacent to the ovary**, not distinctively tubular.
- They can cause pain but are not typically associated with a "tubular" morphology on ultrasound.
*Ectopic pregnancy*
- An ectopic pregnancy would typically present with a **gestational sac** (with or without a fetal pole or yolk sac) outside the uterus, often in the fallopian tube.
- While it can be tubular, it usually shows more complex internal echoes representing pregnancy components, and the clinical picture would involve a **positive pregnancy test** and often acute, unilateral pain.
*Endometrioma*
- An endometrioma is a type of ovarian cyst filled with **endometrial tissue**, often appearing on ultrasound as a **"ground glass" or "chocolate cyst"** with internal echoes due to old blood.
- It would not typically present as a thin-walled, anechoic (purely fluid-filled) tubular structure.
*Tubo-ovarian abscess*
- A tubo-ovarian abscess (TOA) is a **complex inflammatory mass** that typically appears on ultrasound as a **thick-walled, complex structure with internal echoes, septations, or debris**.
- TOA patients usually present with **acute symptoms including fever, elevated white blood cell count**, and severe pelvic pain, rather than the chronic presentation described here.
- The ultrasound description of thin walls and no solid components makes TOA unlikely.
Orthopaedics
1 questions
Q1
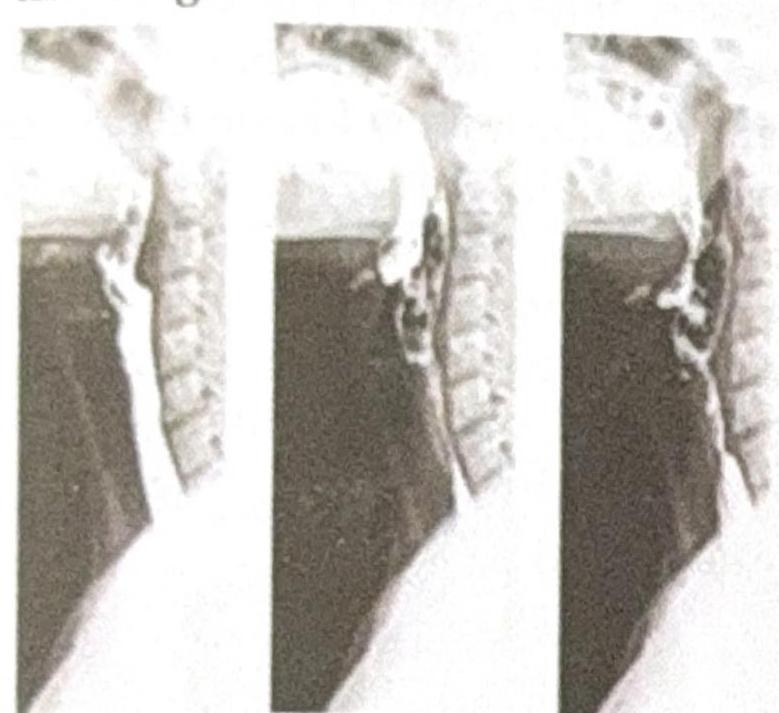
A 35-year-old male presents to the emergency department following a high-speed motor vehicle accident. He complains of severe lower back pain but denies any loss of consciousness or abdominal pain. A lateral X-ray of the lumbar spine is obtained, as shown in the image. The image reveals a horizontal fracture through the vertebral body, extending through the posterior elements. Based on the clinical presentation and imaging findings, what is the most likely diagnosis?
NEET-PG 2024 - Orthopaedics NEET-PG Practice Questions and MCQs
Question 1: A 35-year-old male presents to the emergency department following a high-speed motor vehicle accident. He complains of severe lower back pain but denies any loss of consciousness or abdominal pain. A lateral X-ray of the lumbar spine is obtained, as shown in the image. The image reveals a horizontal fracture through the vertebral body, extending through the posterior elements. Based on the clinical presentation and imaging findings, what is the most likely diagnosis?
A. Burst fracture
B. Compression fracture
C. Chance fracture (Correct Answer)
D. Spondylolisthesis
Explanation: ***Chance fracture***
- A **chance fracture** is characterized by a **horizontal fracture** through the entire vertebral body and posterior elements, including the neural arch, typically caused by a **flexion-distraction mechanism** in accidents like those involving seatbelts (lap belt only), consistent with the high-speed motor vehicle accident scenario.
- The image distinctly shows a fracture line traversing the vertebral body and extending into the posterior elements, which is the hallmark of this type of injury.
*Burst fracture*
- A **burst fracture** involves a comminuted fracture of the vertebral body with **retropulsion of bone fragments** into the spinal canal due to axial loading, which is not clearly depicted here.
- While it can result from high-impact trauma, the characteristic horizontal disruption of both anterior and posterior segments points away from a solely compressive mechanism.
*Compression fracture*
- A **compression fracture** primarily involves the **anterior wedging** or collapse of the vertebral body, resulting from only axial compression forces without significant involvement of the posterior elements.
- The presented image shows a fracture extending through the posterior elements, which is not typical for a simple compression fracture.
*Spondylolisthesis*
- **Spondylolisthesis** is the **anterior slippage of one vertebral body over another**, often due to pars interarticularis defects (spondylolysis) or degenerative changes.
- This condition involves vertebral displacement, not a fresh fracture line across the body and posterior elements as seen in the image.
Pediatrics
2 questions
Q1
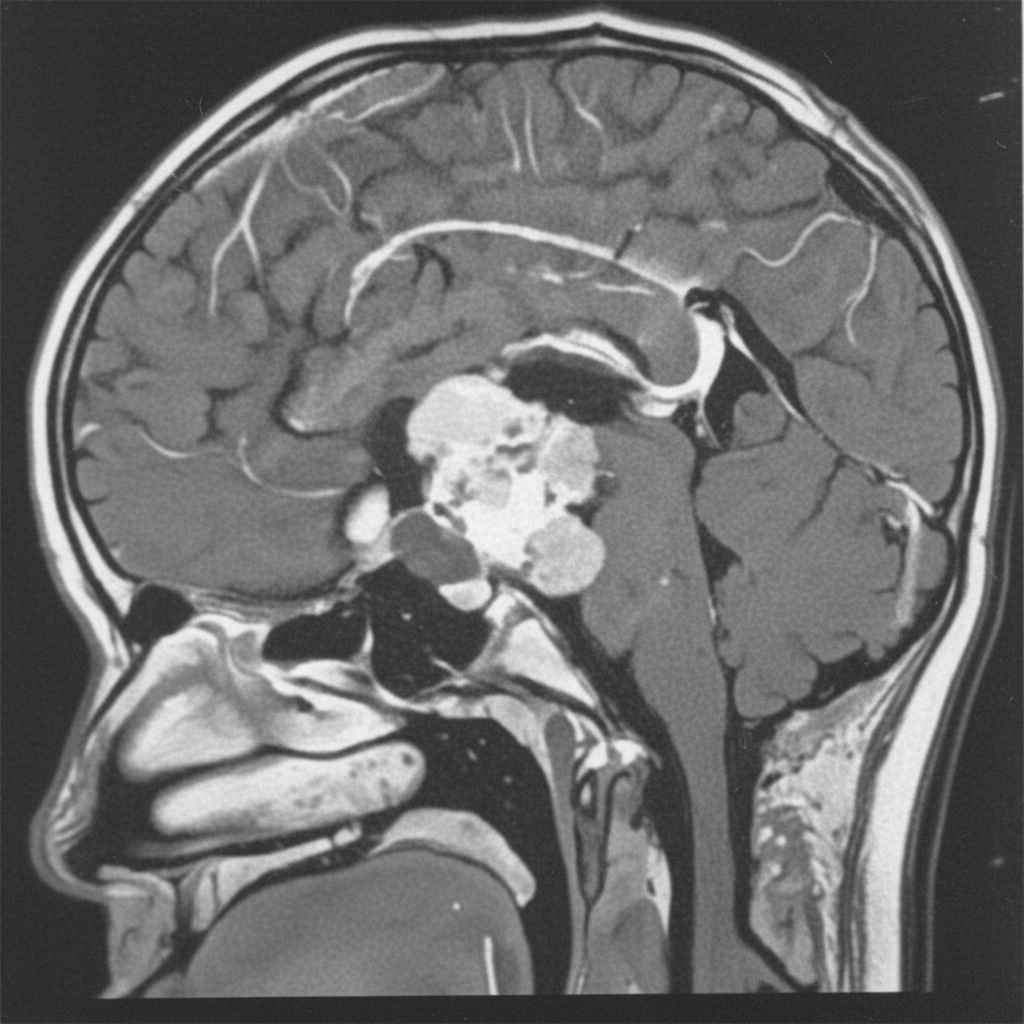
A 12-year-old boy presents with symptoms of headaches, visual disturbances, and growth retardation. An MRI scan is performed, and the image provided shows a cystic mass with both solid and calcified components in the suprasellar region, extending into the third ventricle. Based on the clinical presentation and MRI findings, what is the most likely diagnosis?
Q2
A 2-year-old boy presents with a history of recurrent urinary tract infections, poor urinary stream, and failure to thrive. A voiding cystourethrogram (VCUG) is performed, and the images provided show dilated posterior urethra and a thickened bladder wall with a keyhole appearance. Based on these findings, the diagnosis of posterior urethral valves (PUV) is made. What is the management for this condition?
NEET-PG 2024 - Pediatrics NEET-PG Practice Questions and MCQs
Question 1: A 12-year-old boy presents with symptoms of headaches, visual disturbances, and growth retardation. An MRI scan is performed, and the image provided shows a cystic mass with both solid and calcified components in the suprasellar region, extending into the third ventricle. Based on the clinical presentation and MRI findings, what is the most likely diagnosis?
A. Craniopharyngioma (Correct Answer)
B. Germinoma
C. Meningioma
D. Pituitary adenoma
E. Optic glioma
Explanation: ***Craniopharyngioma***
- This tumor is classically described as having **cystic** and **solid components** with **calcification**, which is evident in the provided MRI image. Its location in the **suprasellar region** and extension into the **third ventricle** are also typical.
- The clinical presentation of **headaches**, **visual disturbances** (due to compression of the optic chiasm), and **growth retardation** (due to hypothalamic-pituitary axis dysfunction) in a 12-year-old boy is highly suggestive of a craniopharyngioma, which commonly affects children and young adults.
*Germinoma*
- While germinomas can occur in the suprasellar region and cause similar endocrine and visual symptoms, they typically appear as **solid, homogeneously enhancing masses** on MRI and are less commonly cystic and calcified.
- They are more common in adolescence and are highly sensitive to radiation therapy, but their imaging characteristics differ from the described lesion.
*Meningioma*
- Meningiomas typically arise from the **arachnoid mater** and are usually **solid, extra-axial masses** that often have a **dural tail sign** on MRI.
- They are less common in children, and while they can calcify, their characteristic imaging features (extra-axial, dural attachment) are not consistent with the described suprasellar, intra-axial cystic mass.
*Pituitary adenoma*
- Pituitary adenomas originate from the **pituitary gland** and are usually located within the sella turcica, extending superiorly. While they can be cystic, **calcification is rare**, and they are more commonly solid and homogeneously enhancing.
- Although they can cause visual disturbances and hormonal imbalances, the prominent cystic-solid appearance with calcification and clear suprasellar origin extending into the third ventricle makes craniopharyngioma a more likely diagnosis in this age group and imaging.
*Optic glioma*
- Optic gliomas (pilocytic astrocytomas) are common **suprasellar tumors in children**, especially those with neurofibromatosis type 1, and can cause visual disturbances and endocrine dysfunction.
- However, they typically appear as **solid, fusiform masses** involving the optic nerve or chiasm with **homogeneous enhancement** and rarely show the characteristic cystic-solid architecture with prominent calcification seen in craniopharyngiomas.
Question 2: A 2-year-old boy presents with a history of recurrent urinary tract infections, poor urinary stream, and failure to thrive. A voiding cystourethrogram (VCUG) is performed, and the images provided show dilated posterior urethra and a thickened bladder wall with a keyhole appearance. Based on these findings, the diagnosis of posterior urethral valves (PUV) is made. What is the management for this condition?
A. Antibiotic prophylaxis and monitoring
B. Endoscopic valve ablation (Correct Answer)
C. Suprapubic cystostomy
D. Observation with follow-up imaging
E. Urinary diversion with vesicostomy
Explanation: ***Endoscopic valve ablation***
- This is the **definitive treatment** for posterior urethral valves (PUV) as it directly addresses the anatomical obstruction.
- Ablating the valves with a **cystoscope** relieves the outflow obstruction, preventing further damage to the bladder and kidneys.
*Antibiotic prophylaxis and monitoring*
- While important for managing recurrent UTIs and preventing future infections in children with PUV, it does **not address the underlying anatomical obstruction**.
- Without surgical intervention, the obstruction would persist, leading to progressive urinary tract damage despite antibiotic use.
*Suprapubic cystostomy*
- This procedure involves placing a catheter directly into the bladder via the abdominal wall to **divert urine**.
- It is typically a **temporary measure** used for initial decompression in severely ill patients or those with complete obstruction, not the definitive management.
*Urinary diversion with vesicostomy*
- Vesicostomy creates an opening between the bladder and abdominal wall for temporary urinary diversion.
- This may be used in **very young infants** or critically ill patients as a temporizing measure, but **endoscopic ablation remains the definitive treatment**.
*Observation with follow-up imaging*
- **Observation is not appropriate** for symptomatic PUV due to the risk of progressive and irreversible renal damage.
- The condition requires **prompt intervention** to relieve the obstruction and prevent long-term complications like renal failure.
Radiology
5 questions
Q1
Identify the investigation being carried out in the image.
Q2
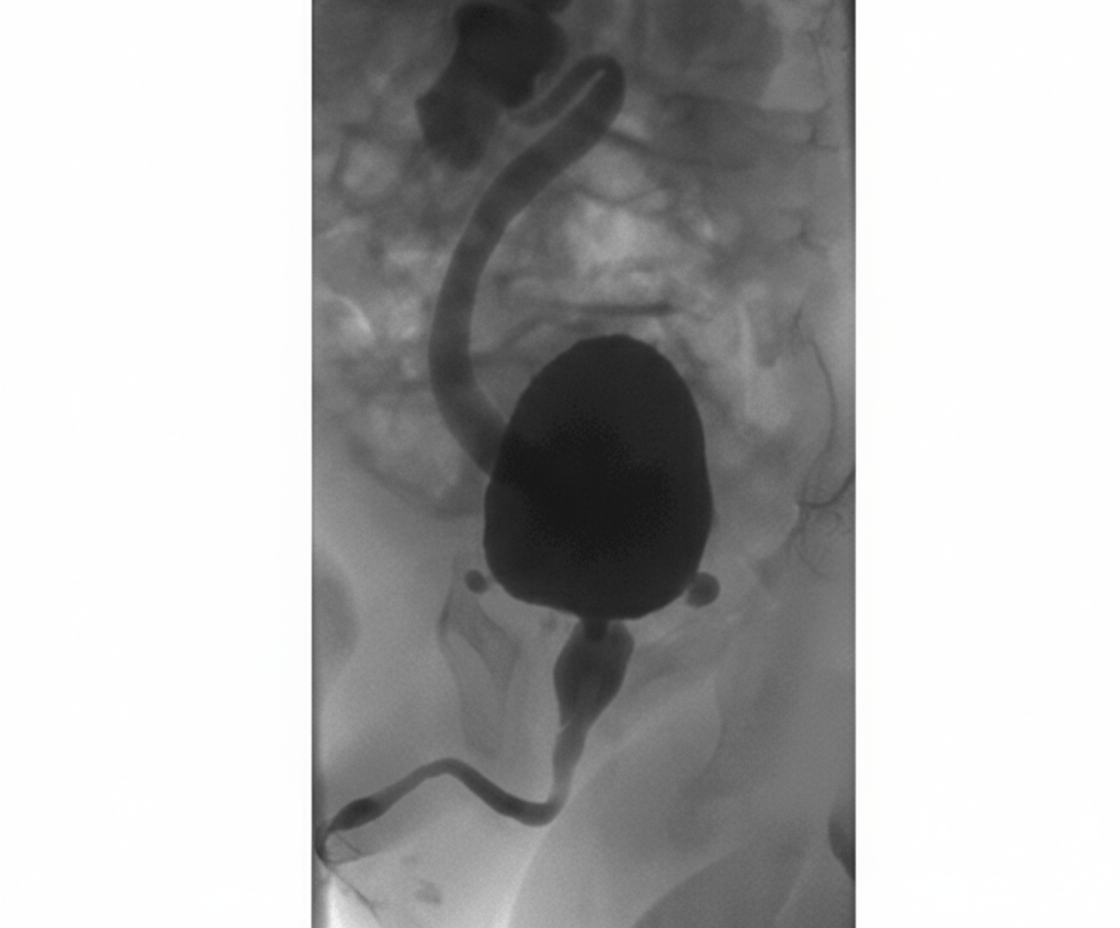
What condition does the MRCP (Magnetic Resonance Cholangiopancreatography) image indicate?
Q3
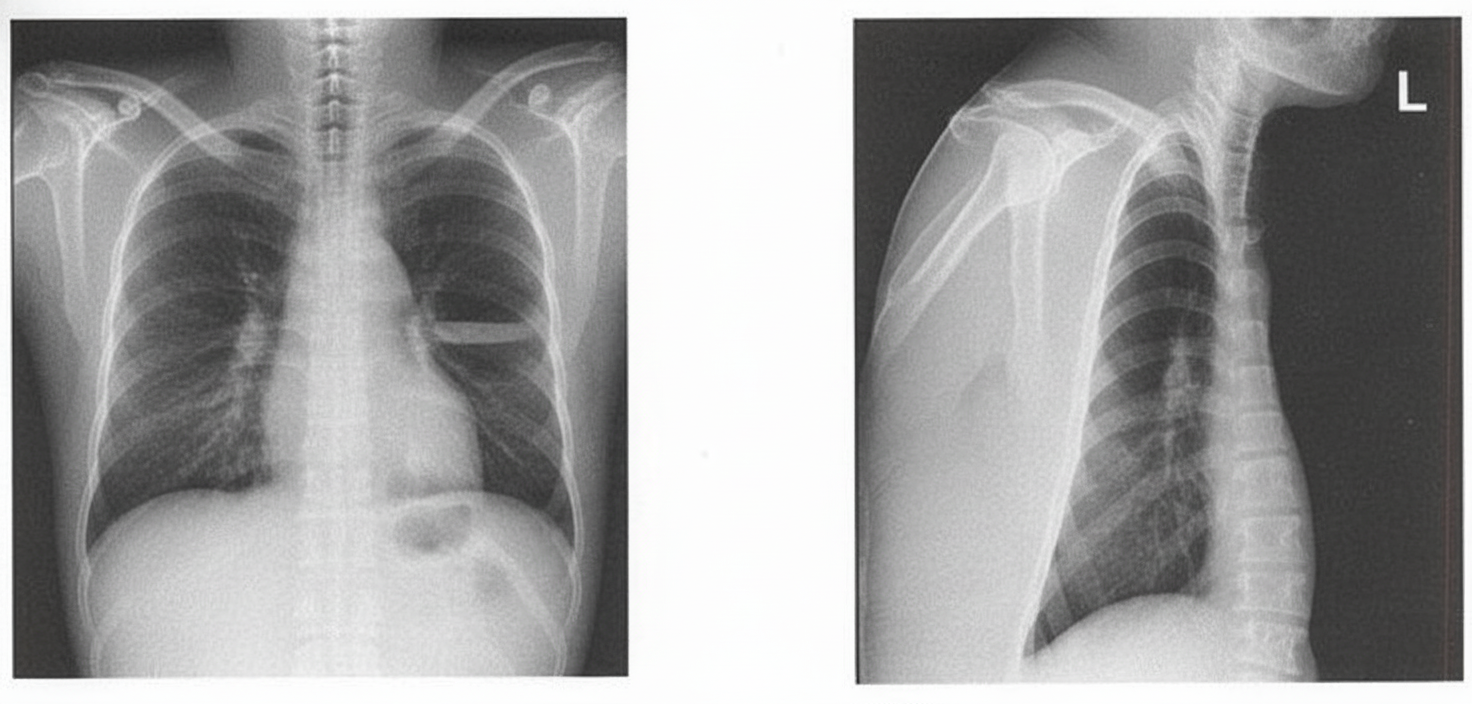
A patient presents with foul-smelling sputum along with breathlessness and fever. Using the X-ray below, identify the diagnosis.
Q4
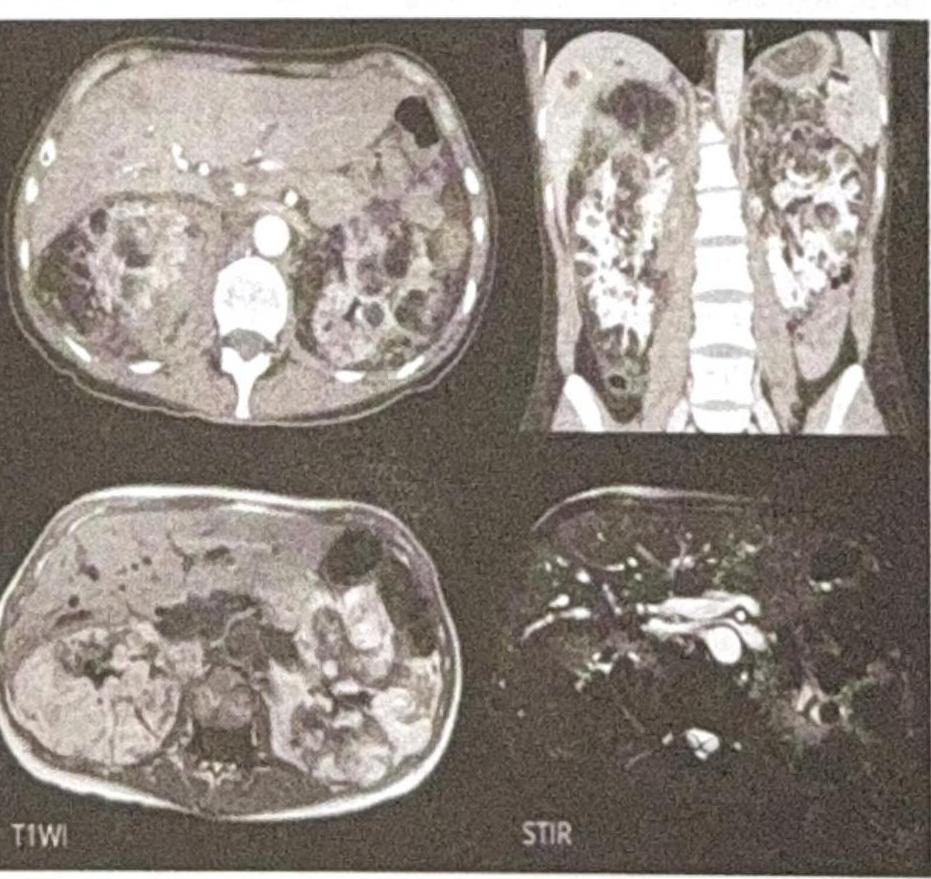
What is the Diagnosis based on the CT Scan given below?
Q5
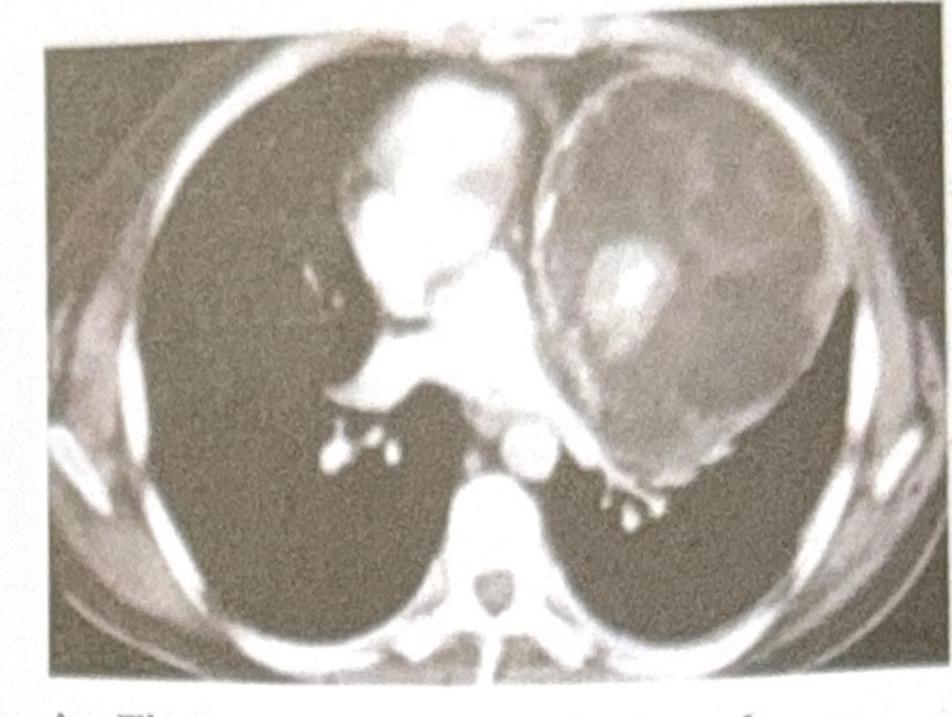
A 25-year-old male presents with chest pain and shortness of breath. A CT scan of the chest is performed, and the image provided shows a large, well-defined mass in the anterior mediastinum. The mass contains both cystic and solid components, along with areas of calcification. Based on the clinical presentation and imaging findings, what is the most likely diagnosis?
NEET-PG 2024 - Radiology NEET-PG Practice Questions and MCQs
Question 1: Identify the investigation being carried out in the image.
A. Fluoroscopy
B. X-ray after alkali ingestion
C. X-ray after acid ingestion
D. Barium Swallow (Correct Answer)
Explanation: ***Barium Swallow***
- The image shows a contrast material, characteristic of **barium**, flowing through the esophagus, captured as a sequence of X-ray images, which is the definition of a barium swallow study.
- This **dynamic imaging** allows for evaluation of swallowing function and esophageal motility.
*Fluoroscopy*
- While a barium swallow uses **fluoroscopy** to visualize the movement of barium, fluoroscopy itself is the technique, not the specific investigation being performed. The image depicts the result of a specific type of fluoroscopic examination.
- Fluoroscopy is a general term for real-time X-ray imaging, whereas "Barium Swallow" specifies the type of study being done on the upper GI tract.
*X-ray after alkali ingestion*
- This scenario would typically involve viewing the effects of **corrosive injury** to the esophagus, which would appear as mucosal damage, narrowing, or perforation. The image does not show these features; instead, it shows smooth passage of contrast.
- There is no visible evidence of an acute or chronic injury pattern consistent with **alkali ingestion**, which often leads to severe burns or strictures.
*X-ray after acid ingestion*
- Similar to alkali ingestion, acid ingestion also causes **corrosive injury**, typically affecting the stomach more severely than the esophagus. The image does not demonstrate these pathological changes.
- The smooth, unobstructed flow of contrast in multiple frames is indicative of normal esophageal function rather than the sequelae of corrosive ingestion.
Question 2: What condition does the MRCP (Magnetic Resonance Cholangiopancreatography) image indicate?
A. Choledochal cyst (Correct Answer)
B. Dilated CBD (Common Bile Duct)
C. Acute cholecystitis
D. Cholangiocarcinoma
Explanation: **Choledochal cyst**
- The MRCP image clearly shows a **cystic dilation** of the common bile duct, which is characteristic of a choledochal cyst.
- This congenital anomaly involves saccular or fusiform dilation of the bile ducts, as depicted by the **balloon-like structure** in the image.
- MRCP is the **gold standard imaging modality** for diagnosing choledochal cysts, providing excellent visualization of the biliary tree anatomy.
*Dilated CBD (Common Bile Duct)*
- While a choledochal cyst is a type of CBD dilation, simply stating "dilated CBD" is not specific enough, as the image shows a distinct **cystic morphology** beyond just uniform dilation.
- Common bile duct dilation can be caused by various factors like stones or strictures, but the **focal, bulbous appearance** points specifically to a cyst.
*Acute cholecystitis*
- Acute cholecystitis typically presents with signs of gallbladder inflammation, such as **gallbladder wall thickening**, pericholecystic fluid, and gallstones, which are not depicted in this MRCP.
- MRCP primarily visualizes the bile ducts and does not typically show the inflammatory changes of the gallbladder wall as clearly as ultrasound or CT.
*Cholangiocarcinoma*
- Cholangiocarcinoma usually manifests as a **stricture** or **mass** within the bile ducts, causing upstream dilation, rather than the isolated cystic dilation seen in the image.
- There is no evidence of an obstructing mass or irregular narrowing within the bile ducts that would suggest a malignancy.
Question 3: A patient presents with foul-smelling sputum along with breathlessness and fever. Using the X-ray below, identify the diagnosis.
A. Pneumothorax
B. Pericardial Effusion
C. Pleural Effusion
D. Lung Abscess (Correct Answer)
Explanation: ***Lung Abscess***
- The combination of **foul-smelling sputum** (indicating anaerobic bacterial infection), breathlessness, and fever is **pathognomonic for lung abscess**
- The X-ray demonstrates a **characteristic air-fluid level** within the lung parenchyma, which is the hallmark radiographic finding of a cavitating lung abscess
- When a lung abscess ruptures into a bronchus, it produces the typical **foul-smelling, purulent sputum** described in this case
- Common causes include aspiration pneumonia, particularly in patients with risk factors like alcoholism, poor dental hygiene, or altered consciousness
*Pleural Effusion*
- While pleural effusion can present with breathlessness and fever, it would **not produce foul-smelling sputum**
- A simple pleural effusion appears as **blunting of the costophrenic angle** or a **meniscus sign**, not an air-fluid level within the lung field
- An empyema (infected pleural effusion) with bronchopleural fistula could theoretically show an air-fluid level, but this would be in the **pleural space**, not within the lung parenchyma, and is much less common than lung abscess
*Pneumothorax*
- Pneumothorax shows **air in the pleural space** with visible lung edge and absent lung markings peripherally
- There would be **no fluid component** and no foul-smelling sputum
- The air-fluid level seen here indicates a cavitary lesion, not a pneumothorax
*Pericardial Effusion*
- Pericardial effusion presents with an **enlarged, globular cardiac silhouette** ("water bottle heart")
- It would **not cause respiratory symptoms** like foul-smelling sputum or the radiographic findings shown
- The pathology is clearly in the **lung field**, not around the heart
Question 4: What is the Diagnosis based on the CT Scan given below?
A. Renal cyst
B. Renal tumor
C. Renal polycystic kidney disease (Correct Answer)
D. Renal angiomyolipoma
Explanation: ***Polycystic kidney disease***
- The CT scan images show **enlarged kidneys** replaced by numerous **cysts of varying sizes**, which is the hallmark appearance of polycystic kidney disease.
- The presence of multiple cysts **bilaterally** and diffusely throughout the renal parenchyma is characteristic of this genetic disorder.
*Renal cyst*
- A single renal cyst is a common benign finding, appearing as a **well-defined, fluid-filled** structure.
- The images clearly demonstrate **multiple cysts** affecting both kidneys, ruling out a solitary renal cyst.
*Renal tumor*
- A renal tumor (e.g., renal cell carcinoma) typically appears as a **solid mass**, often with heterogeneous enhancement after contrast.
- The lesions seen in the image are predominantly **cystic** and multifocal, which is inconsistent with a typical renal tumor.
*Renal angiomyolipoma*
- Renal angiomyolipomas are benign tumors containing **fat, smooth muscle, and blood vessels**, and they characteristically show **macroscopic fat** on CT scans.
- While they can be multiple, especially in tuberous sclerosis, the dominant feature in the image is widespread cystic transformation, not fat-containing solid masses.
Question 5: A 25-year-old male presents with chest pain and shortness of breath. A CT scan of the chest is performed, and the image provided shows a large, well-defined mass in the anterior mediastinum. The mass contains both cystic and solid components, along with areas of calcification. Based on the clinical presentation and imaging findings, what is the most likely diagnosis?
A. Thymoma
B. Lymphoma
C. Teratoma (Correct Answer)
D. Bronchogenic cyst
Explanation: ***Teratoma***
- The presence of a **well-defined anterior mediastinal mass** with **cystic and solid components** and **calcifications** is highly characteristic of a teratoma.
- Teratomas are **germ cell tumors** containing tissues derived from all three embryonic germ layers, which explains their varied composition on imaging.
*Thymoma*
- While thymomas are common in the **anterior mediastinum**, they typically present as **solid masses** and calcifications are less common.
- They are often associated with paraneoplastic syndromes like **myasthenia gravis**, which is not mentioned in this case.
*Lymphoma*
- Lymphoma in the anterior mediastinum often presents as a **lobulated, homogeneous mass**, and can be associated with **lymphadenopathy** elsewhere.
- While it can be large, the specific features of cystic components and calcification are less typical for lymphoma.
*Bronchogenic cyst*
- Bronchogenic cysts are typically **unilocular, fluid-filled cystic lesions** and are usually found in the middle mediastinum or adjacent to the trachea/main bronchi.
- They rarely contain significant solid components or calcifications, unlike the described mass.
About NEET-PG 2024 Questions
This page contains 354 questions from the NEET-PG 2024 paper, organised across 28 subjects for focused practice. Every question comes with the correct answer and a detailed explanation to help you understand the underlying concept. Subject-wise organisation lets you target specific areas and identify which topics carried the most weight in this particular year.
Practising year-wise papers is essential for understanding how the NEET-PG exam evolves — you can spot trending topics, gauge difficulty shifts, and benchmark your readiness against a real paper. To take your preparation further, download the Oncourse app for AI-driven performance insights, spaced repetition of questions you got wrong, and a personalised study plan built around your NEET-PG goals.