All SubjectsAnatomy (1)Anatomy (26)Anesthesiology (9)Biochemistry (26)Community Medicine (10)Dermatology (16)ENT (7)Forensic Medicine (5)General Medicine (1)Internal Medicine (36)Microbiology (23)Obstetrics and Gynecology (13)Ophthalmology (10)Orthopaedics (6)Pathology (1)Pathology (25)Pediatrics (13)Pharmacology (37)Physiology (15)Psychiatry (2)Psychiatry (4)Radiology (11)Surgery (18)
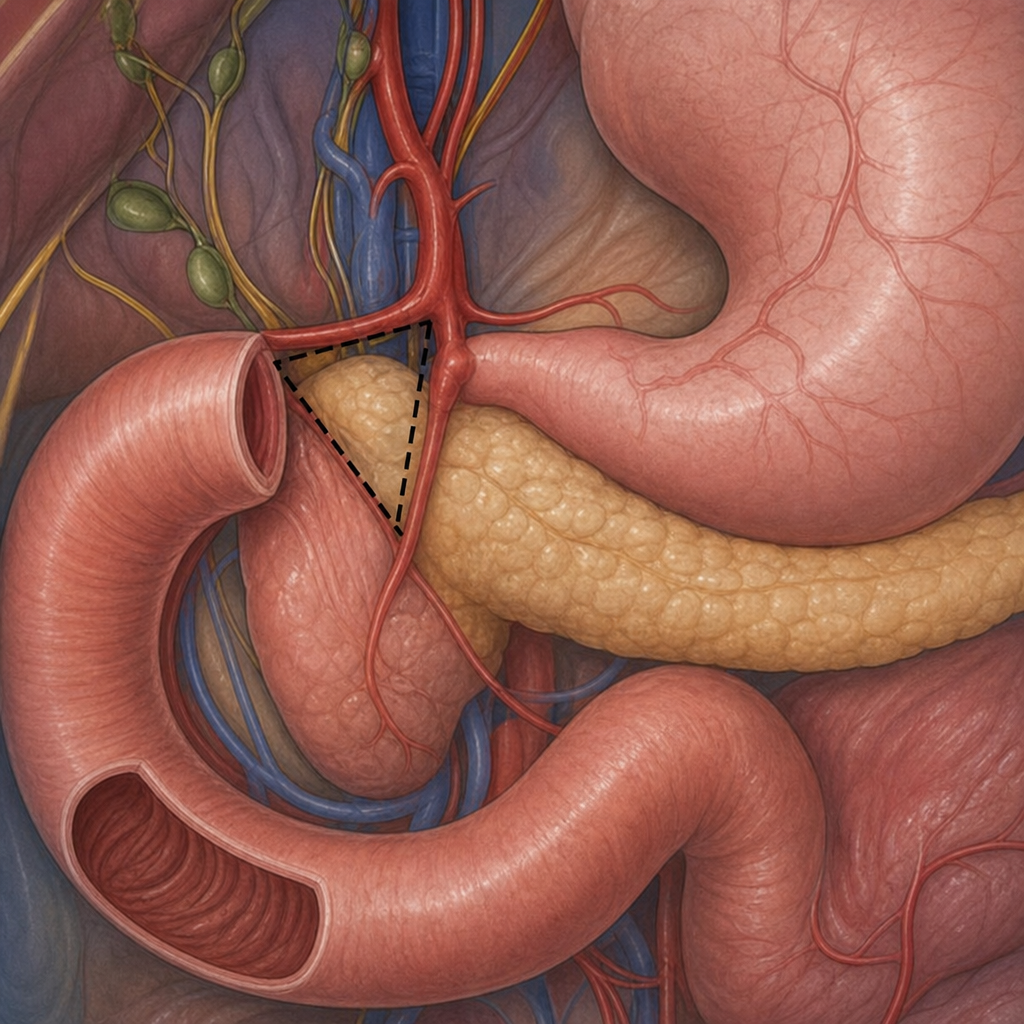
Q11
What is the name of this triangle?
Q12
Most commonly used approach for retrosternal goitre:-
Q13
Which of the following best describes a degloving injury?
Q14
A patient presents with a gradually progressive, painless mass persisting for 10 years. The mass is firm to nodular and shows variable consistency within different areas of the swelling. What is the most probable diagnosis?
Q15
Cushing ulcers are:-
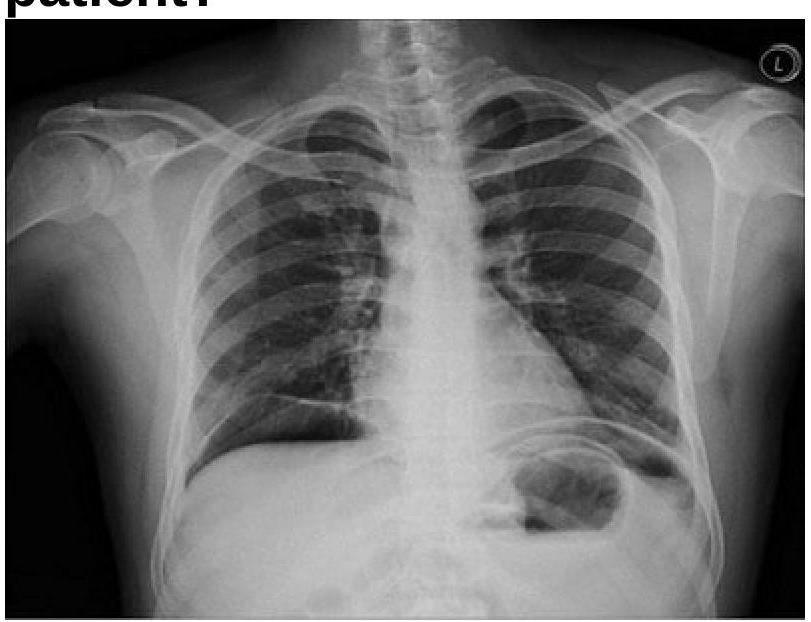
Q16
A 40 years old male was brought emergency with severe abdominal pain. On examination, pulse rate was 112/minute and systolic BP was 80 mmHg. Chest x-ray is given below. What is the most appropriate management?
Q17
Which of the following is true about tenosynovitis of the finger?
Q18
Identify this instrument which is used for harvesting graft from a healthy area in split skin grafting:
