NEET-PG 2019 — Surgery
15 Previous Year Questions with Answers & Explanations
Parathyroid autoimplantation takes place in which muscle?
A patient presented with a history of diplopia and restricted eye movements. What is the most likely diagnosis based on the clinical and CT images?
What type of knot is depicted in the image?
What is the most likely diagnosis for the parotid mass with mixed consistency shown in the image?

CEAP score indicates-
Identify the surgical instrument based on its characteristics: a small, triangular blade used for precise incisions.
Degloving injury involves separation of:-
All of the following statements are true about Frey's Syndrome except
Most commonly used approach for retrosternal goitre:-
Which of the following best describes a degloving injury?
NEET-PG 2019 - Surgery NEET-PG Practice Questions and MCQs
Question 1: Parathyroid autoimplantation takes place in which muscle?
- A. Triceps
- B. Brachioradialis (Correct Answer)
- C. Sartorius
- D. Sternocleidomastoid
Explanation: ***Brachioradialis*** - The **brachioradialis muscle** in the forearm is the preferred site for parathyroid autoimplantation due to its accessibility and favorable blood supply. - This muscle allows for easy **monitoring of parathyroid graft function** and re-exploration if necessary. *Sternocleidomastoid* - While located in the neck, the **sternocleidomastoid muscle** is generally not used for parathyroid autoimplantation due to potential cosmetic concerns and the risk of damage to vital neck structures. - Its proximity to the original parathyroid glands could make it difficult to differentiate native tissue from implanted grafts if future surgery is required. *Triceps* - The **triceps muscle** in the upper arm is a large muscle, but it is not typically chosen for parathyroid autoimplantation. - It is less accessible for routine examination and potential re-exploration compared to the brachial region. *Sartorius* - The **sartorius muscle** is located in the thigh and is not used for parathyroid autoimplantation. - Its distant location from the head and neck region would make monitoring and re-exploration of the graft impractical.
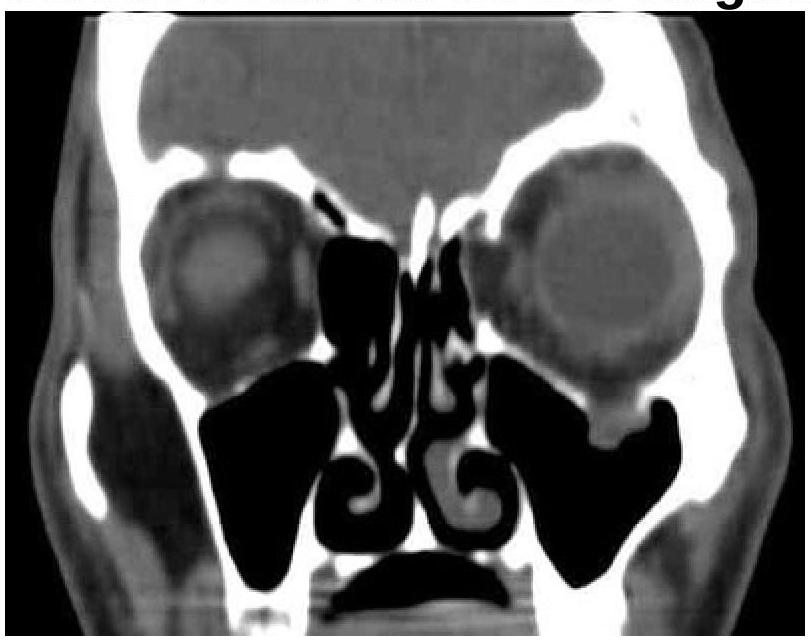
Question 2: A patient presented with a history of diplopia and restricted eye movements. What is the most likely diagnosis based on the clinical and CT images?
- A. Le Fort fracture
- B. Maxillary fracture
- C. Zygomatic fracture
- D. Blowout fracture (Correct Answer)
Explanation: ***Blowout fracture*** - The CT image shows a **fracture of the orbital floor**, with associated **herniation of orbital contents** (fat and inferior rectus muscle) into the maxillary sinus. - This type of fracture commonly causes **diplopia** (due to muscle entrapment) and **restricted eye movements**. *Le Fort fracture* - Le Fort fractures involve the **midface and maxilla** as a whole, typically causing widespread facial instability. - They are classified into three types (I, II, III), none of which are exclusively characterized by an isolated orbital floor fracture with muscle entrapment. *Maxillary fracture* - While an orbital floor fracture involves the maxilla, a "maxillary fracture" is a broad term and does not specifically describe the characteristic features of **orbital content prolapse** and their resulting symptoms. - Isolated maxillary fractures might not cause diplopia or restricted eye movements unless they directly involve the orbit. *Zygomatic fracture* - A zygomatic fracture (either isolated or as part of a zygomaticomaxillary complex fracture) primarily affects the **cheekbone**. - While it can involve the orbital rim, it typically presents with **facial asymmetry**, **numbness** in the infraorbital nerve distribution, and sometimes **trismus**, rather than isolated muscle entrapment causing diplopia, as seen in the image.
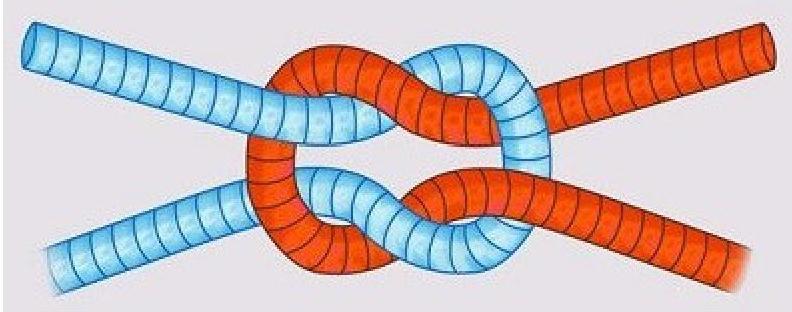
Question 3: What type of knot is depicted in the image?
- A. Half hitch
- B. Granny knot (Correct Answer)
- C. Surgeon’s knot
- D. Reef knot
Explanation: ***Granny knot*** - The image shows a knot where the two half-knots are tied in the **same direction** (left over right, then left over right again, or vice versa), causing it to be unstable and slip. - This instability makes it less secure than a reef knot, as the two end pieces emerge parallel but on opposite sides of the loop. - The granny knot is an **insecure knot** that should be avoided in surgery as it can spontaneously untie. *Surgeon's knot* - A surgeon's knot involves an **extra throw** (double wrap) around the first loop to increase friction and make it more secure, which is not depicted here. - It is typically used to ensure that the first throw holds tension while the second throw is being tied. *Reef knot* - A reef knot (or square knot) is formed by tying two half-knots in **opposite directions** (left over right, then right over left), which creates a flat, stable, and secure knot. - In a reef knot, the two end pieces emerge parallel and on the same side of the loop, unlike the granny knot. *Half hitch* - A half hitch is a simple overhand knot around a standing part of the rope, used as a single throw or in combination with other knots. - It is not the same as the double-throw configuration shown in the image.
Question 4: What is the most likely diagnosis for the parotid mass with mixed consistency shown in the image?
- A. Pleomorphic adenoma (Correct Answer)
- B. Sebaceous cyst
- C. Dermoid cyst
- D. None of the options
Explanation: ***Pleomorphic adenoma*** - The **mixed consistency** of the parotid mass indicates a **benign tumor**, predominantly of epithelial and mesenchymal origin, typical of pleomorphic adenomas. - This type of tumor is usually **pain-free** and can exhibit a **soft** and **firm** texture on examination [1]. *Sebaceous cyst* - Typically presents as a **smooth, fluctuant nodule** and usually has a **firm consistency** rather than mixed. - Generally not seen as a parotid mass; usually found on the skin in areas with sebaceous glands. *Dermoid cyst* - Generally presents as a **well-defined, soft, and mobile mass**, not commonly associated with mixed consistency. - Often contains **keratin** and has a more homogenous consistency rather than the mixed characteristics of pleomorphic adenoma. *All* - As not all options are suitable for the description of a **mixed consistency parotid mass**, this option is incorrect. - Only **pleomorphic adenoma** aligns with the specific clinical presentation detailed in the question [1]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Head and Neck, pp. 751-753.
Question 5: CEAP score indicates-
- A. Atrial disorders
- B. Venous disorder (Correct Answer)
- C. Trauma disorder
- D. Neurological disorder
Explanation: ***Venous disorder*** - The **CEAP classification** is a widely recognized system used to categorize and describe chronic venous disorders. The acronym stands for **Clinical, Etiological, Anatomical, and Pathophysiological** factors. - It provides a standardized framework for clinicians to classify the severity and characteristics of **venous disease**, ranging from spider veins to active ulcers. *Atrial disorders* - **Atrial disorders** refer to conditions affecting the atria of the heart, such as **atrial fibrillation** or **atrial flutter**. - These are cardiovascular conditions distinct from venous disorders, which involve the veins (blood vessels returning blood to the heart). *Neurological disorder* - A **neurological disorder** is a condition affecting the **nervous system**, including the brain, spinal cord, and nerves. - The CEAP classification is specifically designed for vascular conditions and has no direct relevance to neurological diseases. *Trauma disorder* - A **trauma disorder** is a condition resulting from a **physically or psychologically traumatic event**. - While trauma can sometimes lead to venous issues (e.g., deep vein thrombosis from immobilization), the CEAP score itself is a classification system for chronic venous disease, not for traumatic conditions in general.
Question 6: Identify the surgical instrument based on its characteristics: a small, triangular blade used for precise incisions.
- A. Blade no. 15
- B. Blade no. 10
- C. Blade no. 11 (Correct Answer)
- D. Blade no. 12
Explanation: ***Blade no. 11*** - This blade has a **triangular shape** with a strong, pointed tip, making it ideal for **stab incisions** and precise, short cuts. - Its design allows for sharp, accurate penetration, often used in procedures requiring **minimal tissue disruption**. *Blade no. 15* - This is a small, curved blade, primarily used for **fine, precise cuts** in superficial tissues. - Its small size and rounded belly make it suitable for tasks like excising skin lesions or making incisions in delicate areas, not for triangular stab incisions. *Blade no. 10* - The No. 10 blade has a **large, curved cutting edge** and is generally used for making large incisions in skin and muscle. - It is not designed for precise, triangular stab incisions, but rather for broader, sweeping cuts. *Blade no. 12* - This blade is **sickle-shaped** with the cutting edge on the inside curve, used primarily for mucogingival surgery or removing sutures. - Its unique shape allows it to get into tight spaces and cut from a different angle, but it does not have a triangular tip for precise stab incisions.
Question 7: Degloving injury involves separation of:-
- A. Skin
- B. Everything above from bone
- C. Skin + Subcutaneous tissue
- D. Skin + Fascia + Subcutaneous tissue (Correct Answer)
Explanation: ***Skin + Fascia + Subcutaneous tissue*** - A **degloving injury** involves the traumatic separation of skin, subcutaneous tissue, and **superficial fascia** from the underlying deep fascia and muscle structures. - The separation typically occurs at the plane between the **superficial fascia** and **deep fascia**, creating the characteristic "degloved" appearance with loss of multiple tissue layers. *Skin + Subcutaneous tissue* - This option is incomplete as it fails to explicitly mention the **superficial fascia** component that is also involved in degloving injuries. - While anatomically the subcutaneous tissue includes fascial elements, the complete description should specifically include **fascia** as a separate component. *Skin* - This option is severely incomplete as degloving injuries involve much more than just the **epidermal and dermal layers**. - A true degloving injury must include separation of the **subcutaneous tissue** and **superficial fascia** to create the characteristic tissue defect. *Everything above from bone* - This description is too extensive and would represent a **complex avulsion** or **near-amputation** rather than a typical degloving injury. - Degloving specifically refers to separation at the **superficial-deep fascial plane**, not removal of all overlying tissues including muscle and deep fascia.
Question 8: All of the following statements are true about Frey's Syndrome except
- A. Less chances with enucleation than parotidectomy
- B. Gustatory sweating
- C. Aberrant misdirection of parasympathetic fibers of auriculotemporal nerve
- D. Sympathetic nerve involvement is the primary cause (Correct Answer)
Explanation: ***Sympathetic nerve involvement is the primary cause*** - **This is FALSE (Correct answer for EXCEPT question)** - Frey's syndrome is **NOT** caused by sympathetic nerve involvement - The primary cause is **aberrant regeneration of severed PARASYMPATHETIC fibers** of the auriculotemporal nerve - These parasympathetic fibers mistakenly re-innervate sweat glands (which are sympathetically innervated) instead of the parotid gland - This misdirection causes gustatory sweating during meals *Less chances with enucleation than parotidectomy* - **TRUE** - Enucleation is a less extensive procedure compared to complete parotidectomy - Less tissue removal means less nerve disruption and lower risk of auriculotemporal nerve damage - The risk of Frey's syndrome is directly proportional to the extent of parotid tissue removal *Gustatory sweating* - **TRUE** - This is the hallmark symptom of Frey's syndrome - Characterized by sweating on the skin over the parotid region in response to salivary stimuli (smelling, seeing, or eating food) - Results from misdirected parasympathetic fibers stimulating sweat glands instead of salivary tissue *Aberrant misdirection of parasympathetic fibers of auriculotemporal nerve* - **TRUE** - This is the correct pathophysiological mechanism underlying Frey's syndrome - Following injury to the auriculotemporal nerve during parotid surgery, regenerating parasympathetic secretomotor fibers become misdirected - These fibers intended for the parotid gland instead innervate sweat glands in the overlying skin
Question 9: Most commonly used approach for retrosternal goitre:-
- A. Transthoracic second intercostal space
- B. Axillary approach
- C. Trans-sternal through anterior mediastinum
- D. Transcervical (Correct Answer)
Explanation: ***Transcervical*** - The transcervical approach is the **most common and preferred method** for resecting retrosternal goitres, as the majority can be delivered through the **thoracic inlet**. - This approach minimizes morbidity and avoids the need for a **sternotomy** in most cases. *Transthoracic second intercostal space* - This approach is typically reserved for **mediastinal masses** or procedures requiring direct access to the **pleural cavity**, which is generally not necessary for retrosternal goitres. - It would involve a more invasive incision than typically required for a goitre that can be delivered transcervically. *Axillary approach* - The axillary approach is primarily used for **lymph node dissection** in breast cancer or for certain **thoracoscopic procedures**, not for accessing the thyroid gland for retrosternal goitre removal. - Its anatomical location does not provide adequate exposure to the **cervical and mediastinal structures** involved in a retrosternal goitre. *Trans-sternal through anterior mediastinum* - A trans-sternal approach (sternotomy) is a **major surgical procedure** typically reserved for very large, irreducible retrosternal goitres that have significant **mediastinal extension** or are adherent to surrounding structures. - It is avoided whenever possible due to increased morbidity and longer recovery compared to the transcervical approach, making it less commonly used overall.
Question 10: Which of the following best describes a degloving injury?
- A. Separation of only the skin layer
- B. Separation of skin and subcutaneous tissue without fascia involvement
- C. Exposure of tendons without skin and fascia separation
- D. Separation of skin, subcutaneous tissue, and fascia with tendon exposure (Correct Answer)
Explanation: ***Separation of skin, subcutaneous tissue, and fascia with tendon exposure*** - A **degloving injury** is characterized by the avulsion of skin, subcutaneous tissue, and fascia from the underlying muscle and connective tissue due to **shearing forces**. - This extensive separation often exposes deeper structures like **tendons**, bones, or neurovascular bundles in severe cases, though tendon exposure is not universally present in all degloving injuries. - The key feature is the **separation of multiple tissue layers** including fascia, which distinguishes it from superficial injuries. - Can be **open** (complete skin avulsion) or **closed** (Morel-Lavallée lesion with intact skin but underlying separation). *Separation of only the skin layer* - This description is incomplete as a degloving injury involves deeper layers beyond just the epidermal and dermal skin layers. - Simple skin separation or abrasion does not involve the extensive avulsion of **subcutaneous tissue and fascia** seen in degloving. *Separation of skin and subcutaneous tissue without fascia involvement* - While degloving involves skin and subcutaneous tissue separation, the crucial element of **fascia involvement** is missing from this description. - The tearing and separation at the **fascial plane** is key to the classification of a true degloving injury, distinguishing it from less severe avulsion injuries. *Exposure of tendons without skin and fascia separation* - Tendon exposure without concomitant skin and fascia separation would typically describe an **open wound** or deep laceration, not a degloving injury. - A degloving injury's hallmark is the **shearing force** that detaches extensive layers of soft tissue from their underlying attachments, not isolated tendon exposure.