NEET-PG 2019 — Radiology
8 Previous Year Questions with Answers & Explanations
Boot shape of heart in TOF is due to:
Identify the condition based on the provided image.
Identify the condition in the image below?
Identify the radiological procedure shown in the image?

Which of the following is water soluble contrast?
A 75-year-old female has chronic backache. X-ray of the spine is shown. What is the most likely diagnosis?

Gas absent from intestine (gasless abdomen) on x-ray is seen in which condition?
An image of a newborn infant is shown. What is the most likely diagnosis?

NEET-PG 2019 - Radiology NEET-PG Practice Questions and MCQs
Question 1: Boot shape of heart in TOF is due to:
- A. Right ventricular hypertrophy (Correct Answer)
- B. Enlargement of the left atrium
- C. Enlargement of the right atrium
- D. Hypertrophy of both ventricles
Explanation: ***Right ventricular hypertrophy*** - The characteristic **boot-shaped heart (coeur en sabot)** seen in Tetralogy of Fallot (TOF) on a chest X-ray is primarily due to **right ventricular hypertrophy** and the small pulmonary artery. - The hypertrophied right ventricle lifts the cardiac apex, while the concavity in the area of the pulmonary artery (due to **pulmonary stenosis**) gives the heart its distinctive shape. *Enlargement of the left atrium* - Left atrial enlargement is not a feature of **Tetralogy of Fallot**; in fact, chronic pulmonary outflow obstruction often leads to a relatively normal or small left atrium. - This condition involves right-sided heart abnormalities, and left atrial enlargement would suggest increased left-sided pressures, which are not typical for TOF. *Enlargement of the right atrium* - While right atrial enlargement can occur in severe cases of TOF due to increased resistance to blood flow, it is **right ventricular hypertrophy** that is the primary determinant of the classic boot-shaped cardiac silhouette. - Right atrial enlargement alone does not create the specific "boot" appearance which is largely due to the ventricular contour. *Hypertrophy of both ventricles* - In Tetralogy of Fallot, the primary ventricular abnormality is **right ventricular hypertrophy**, driven by the need to pump blood through a stenosed pulmonary artery. - The left ventricle typically maintains a normal size and function, as it primarily pumps into the systemic circulation and is not directly affected by the primary defects in the same way as the right ventricle.
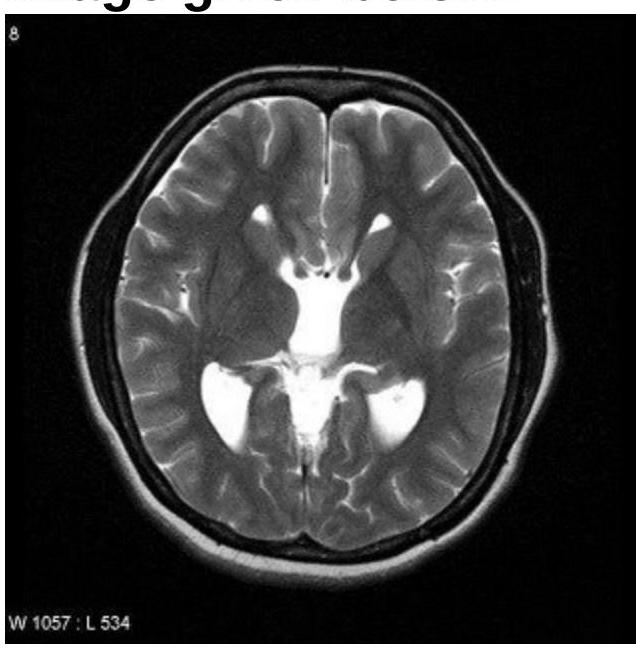
Question 2: Identify the condition based on the provided image.
- A. Callosal dysgenesis (Correct Answer)
- B. Dandy-Walker syndrome
- C. Aicardi syndrome
- D. Septo-optic dysplasia
Explanation: ***Callosal dysgenesis*** - The image shows **colpocephaly**, characterized by **dilatation of the posterior horns** of the lateral ventricles and narrowing of the anterior horns. This is a classic MRI finding in callosal dysgenesis. - The absence or partial formation of the **corpus callosum** leads to a high-riding third ventricle and parallel lateral ventricles, which are often visualized alongside colpocephaly. *Dandy-Walker syndrome* - Characterized by a **cystic dilatation of the fourth ventricle** that fills the posterior fossa, leading to an upward displacement of the tentorium. - This condition involves agenesis or hypoplasia of the **cerebellar vermis**, which is not depicted in this image. *Aicardi syndrome* - Aicardi syndrome is characterized by the triad of **agenesis of the corpus callosum**, **chorioretinal lacunae**, and **infantile spasms**. - While it includes agenesis of the corpus callosum, the image alone does not provide evidence of the ocular or seizure components of Aicardi syndrome. *Septo-optic dysplasia* - This condition is defined by the **triad of optic nerve hypoplasia**, **pituitary hormone abnormalities**, and **midline brain defects**, specifically hypoplasia or absence of the septum pellucidum. - The image does not show features specific to optic nerve hypoplasia or the typical midline cysts or absent septum pellucidum characteristic of septo-optic dysplasia.
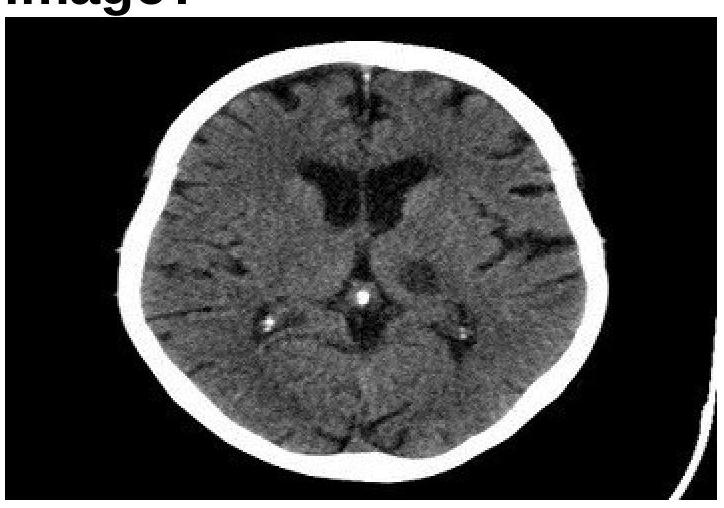
Question 3: Identify the condition in the image below?
- A. Lacunar infarct (Correct Answer)
- B. Embolic infarct
- C. Thrombotic infarct
- D. Intracerebral hemorrhage
Explanation: ***Lacunar infarct*** - The image displays a small, well-demarcated **hypodensity** (darker area) in the basal ganglia region, characteristic of a lacunar infarct. - Lacunar infarcts are typically caused by **occlusion of small perforating arteries** and result in small, deep infarcts, often appearing as precise, round or ovoid lesions on CT. *Embolic infarct* - Embolic infarcts tend to be **larger**, wedge-shaped, and often extend to the cortical surface, unlike the deep, small lesion seen. - They are commonly associated with a **cardiac source** or large artery atherosclerosis leading to distal embolization. *Thrombotic infarct* - Thrombotic infarcts are usually **larger** areas of infarction due to occlusion of a major artery, often preceded by symptoms like TIAs. - While they also appear hypodense, they are typically **more extensive** and less precisely defined than a lacunar infarct in the early stages. *Intracerebral hemorrhage* - Intracerebral hemorrhage would appear as a **hyperdense** (bright white) area on a non-contrast CT scan due to the presence of acute blood. - The image clearly shows a **hypodense lesion**, ruling out acute hemorrhage.
Question 4: Identify the radiological procedure shown in the image?
- A. Barium meal follow through (Correct Answer)
- B. Barium enema
- C. Enteroclysis
- D. Proctography
Explanation: ***Barium meal follow through*** - The image shows opacification of the stomach and the entire small bowel loops via oral uptake of a contrast agent, which is characteristic of a **barium meal follow-through**. - This procedure tracks the passage of **barium** from the esophagus, stomach, and duodenum, through the jejunum and ileum, to assess the **small intestine's morphology and function**. *Barium enema* - A **barium enema** involves introducing contrast material rectally to visualize the **colon and rectum**, which is not depicted in this image. - The primary structures opacified in a barium enema are the **large intestine**, not the stomach and small bowel as seen here. *Enteroclysis* - **Enteroclysis** is a specialized study of the small bowel where contrast is directly instilled into the **duodenum** or **proximal jejunum** via a nasoenteric tube. - While it visualizes the small bowel, the image shows oral contrast progression from the stomach, not direct jejunal intubation. *Proctography* - **Proctography**, also known as defecography, is a dynamic study focused specifically on the **rectum and anal canal** during defecation. - This procedure is highly specific to the distal gastrointestinal tract for assessing anorectal function and does not visualize the stomach or extensive small bowel loops.
Question 5: Which of the following is water soluble contrast?
- A. Barium
- B. Iodine (Correct Answer)
- C. Bromine
- D. Calcium
Explanation: ***Iodine*** - **Iodinated contrast media** (containing iodine atoms) are the most commonly used **water-soluble contrast agents** in medical imaging. - Examples include **non-ionic iodinated compounds** (iohexol, iopamidol, iopromide) and **ionic compounds** (diatrizoate, iothalamate). - The **iodine atoms** provide radiodensity (X-ray attenuation), while the organic molecular structure ensures **water solubility**. - These agents are safely excreted by the kidneys and are used intravenously for CT angiography, intravenous urography, and contrast-enhanced CT scans. *Barium* - **Barium sulfate** is a **water-insoluble** compound used as an oral or rectal contrast agent for imaging the gastrointestinal tract. - It remains in the GI lumen and is not absorbed; if extravasated into soft tissues, it can cause significant inflammatory reactions. - Used for barium swallow, barium meal, barium follow-through, and barium enema studies. *Bromine* - **Bromine** is not used as a contrast agent in medical imaging due to its high toxicity and unsuitability for diagnostic purposes. - It does not form stable, non-toxic water-soluble compounds appropriate for clinical imaging. *Calcium* - **Calcium** is a natural component of bone and provides intrinsic radiodensity on plain X-rays. - It is not administered as an exogenous contrast agent for diagnostic imaging purposes.
Question 6: A 75-year-old female has chronic backache. X-ray of the spine is shown. What is the most likely diagnosis?
- A. Osteoporosis (Correct Answer)
- B. Spondylodiscitis
- C. Pott's spine
- D. Spondylolisthesis
Explanation: ***Osteoporosis*** - The X-ray shows diffuse **osteopenia** (reduced bone density) and **vertebral compression fractures**, particularly visible in the lateral view, which are characteristic findings in elderly patients with osteoporosis and chronic backache. - The vertebral bodies appear **demineralized** and some exhibit a loss of height, suggesting collapse due to weakened bone structure. *Spondylodiscitis* - This condition involves **inflammation of the vertebral body and adjacent intervertebral disc**, typically showing **erosions** of the vertebral endplates and **narrowing of the disc space** on X-ray, which are not clearly evident here as the primary issue. - While it can cause back pain, the dominant finding on this X-ray is widespread bone density loss and fractures, rather than localized infection-related changes. *Pott's spine* - Pott's spine (**tuberculous spondylitis**) is a form of osteomyelitis that causes **destruction of vertebral bodies** and adjacent discs, often leading to a **gibbus deformity** (sharp posterior angulation of the spine). - The X-ray does not show extensive vertebral destruction, paraspinal abscess formation, or typical kyphotic deformity associated with Pott's spine. *Spondylolisthesis* - Spondylolisthesis is characterized by the **forward slippage of one vertebral body over another**, often due to a defect in the pars interarticularis. - While there may be some degenerative changes, there is no clear evidence of significant anterior translation of a vertebral body on the lateral X-ray that would indicate spondylolisthesis.
Question 7: Gas absent from intestine (gasless abdomen) on x-ray is seen in which condition?
- A. Ulcerative colitis
- B. Intussusception
- C. Acute pancreatitis (Correct Answer)
- D. Necrotizing enterocolitis
Explanation: ***Acute pancreatitis*** - In **severe acute pancreatitis**, a **gasless or relatively gasless abdomen** may be seen due to profound **ileus** with fluid accumulation displacing intestinal gas. - The marked inflammatory process can lead to complete loss of intestinal motility and fluid sequestration (third-spacing), resulting in minimal visible bowel gas on X-ray. - **Note**: Classic signs include **sentinel loop sign** (dilated jejunal loop) or **colon cut-off sign**, but in severe cases with massive ascites or fluid collections, a gasless pattern may occur. *Ulcerative colitis* - Typically presents with **dilated loops of large bowel** with visible gas and **toxic megacolon** in severe cases. - Inflammatory changes cause bowel wall thickening, but gas is usually **present and often increased**. *Intussusception* - May show a **target sign** or **meniscus sign** on imaging, with bowel loops dilated proximal to the obstruction. - Gas is typically **present** within the bowel or proximal to the invagination, not absent from the entire abdomen. *Necrotizing enterocolitis* - Characterized by **pneumatosis intestinalis** (gas in the bowel wall) and **portal venous gas**, features directly contradicting a gasless abdomen. - Shows dilated loops with gas and evidence of bowel wall necrosis - **gas is prominently present**.
Question 8: An image of a newborn infant is shown. What is the most likely diagnosis?
- A. Infant of diabetic mother (Correct Answer)
- B. Beckwith Wiedemann syndrome
- C. Congenital hypothyroidism
- D. IUGR baby
Explanation: ***Infant of diabetic mother*** - The image depicts a **large for gestational age (LGA)** or **macrosomic** infant with a **plethoric appearance** and significant subcutaneous fat, which are classic signs of an infant of a diabetic mother. - Maternal hyperglycemia leads to fetal hyperinsulinemia, causing increased fetal growth and fat deposition. *Beckwith Wiedemann syndrome* - While infants with Beckwith-Wiedemann syndrome can be LGA, they typically present with characteristic features such as **macroglossia**, **omphalocele**, **ear creases/pits**, and **hemihyperplasia**, which are not clearly evident in this image. - The overall appearance of diffuse adiposity is more consistent with uncontrolled maternal diabetes. *Congenital hypothyroidism* - Infants with congenital hypothyroidism are often **hypotonic**, have a **hoarse cry**, prolonged jaundice, and a characteristic **coarse facial appearance** with a large tongue and umbilical hernia, and are typically *not* macrosomic. - The appearance in the image does not align with the typical features of congenital hypothyroidism. *IUGR baby* - An **intrauterine growth restriction (IUGR)** baby is small for gestational age (SGA) due to various factors impeding fetal growth. - The infant in the image is clearly **macrosomic**, and not small, directly contradicting the definition of IUGR.