NEET-PG 2019 — Pediatrics
11 Previous Year Questions with Answers & Explanations
Which viral infection is known to cause a condition resembling erythroblastosis?
Bimanual grip is seen at what age?
What is the definition of severe acute malnutrition according to WHO criteria?
What should be the correct treatment for a 14-year-old child with newly diagnosed Juvenile Rheumatoid Arthritis?
Fast breathing in a 6-month-old infant is taken as:
Which among the following is NOT part of the classic clinical triad of necrotizing enterocolitis?
Congenital Rubella Syndrome includes all except
Which of the following is most specific for congenital Rubella syndrome?
Bilateral grasp is seen at what age?
Comment on the diagnosis of the patient?
NEET-PG 2019 - Pediatrics NEET-PG Practice Questions and MCQs
Question 1: Which viral infection is known to cause a condition resembling erythroblastosis?
- A. EBV
- B. CMV
- C. Parvovirus B19 (Correct Answer)
- D. HSV
Explanation: ***Parvovirus B19*** - **Parvovirus B19** has a specific tropism for **erythroid progenitor cells** in the bone marrow. - In the fetus, congenital infection causes **severe anemia** due to destruction of red blood cell precursors, leading to **hydrops fetalis** with massive compensatory erythropoiesis. - This results in circulating **nucleated red blood cells (erythroblasts)**, hepatosplenomegaly from extramedullary hematopoiesis, and severe anemia - a picture closely **resembling erythroblastosis fetalis**. - Unlike the immune-mediated hemolysis in Rh isoimmunization, parvovirus causes direct viral destruction of erythroid precursors with similar clinical manifestations. *CMV* - **Cytomegalovirus (CMV)** is the most common congenital infection and can cause hepatosplenomegaly, jaundice, and thrombocytopenia. - However, CMV typically causes **direct hyperbilirubinemia** from hepatocellular damage rather than the hemolytic anemia pattern seen in erythroblastosis. - While CMV can affect hematopoiesis, it does not characteristically produce the massive erythroblast response and hydrops pattern typical of erythroblastosis fetalis. *EBV* - **Epstein-Barr virus (EBV)** primarily causes **infectious mononucleosis** in older children and adults, with atypical lymphocytosis. - EBV is rare in neonates and does not cause fetal hydrops or an erythroblastosis-like syndrome. - Associated with lymphoproliferative disorders and post-transplant complications rather than fetal anemia. *HSV* - **Herpes simplex virus (HSV)** causes disseminated neonatal infection with encephalitis, hepatitis, and mucocutaneous lesions. - HSV does not have tropism for erythroid precursors and does not cause the anemia, hydrops, or erythroblastosis-like picture. - Typically acquired perinatally rather than causing congenital infection with hematologic manifestations.
Question 2: Bimanual grip is seen at what age?
- A. 5 months
- B. 7 months
- C. 4 months
- D. 6 months (Correct Answer)
Explanation: ***6 months*** - **Bimanual grip**, which involves using both hands to grasp an object, typically develops around **6 months of age**. - This milestone marks the ability to bring objects to the midline and use both hands cooperatively. *4 months* - At **4 months**, infants typically start to reach for objects with one hand but do not yet consistently demonstrate a coordinated **bimanual grip**. - They are more likely to swipe at objects or grasp with a **primitive palmar grasp** in one hand. *5 months* - While infants at **5 months** show increasing dexterity and may bring objects to the midline, a full, consistent **bimanual grip** is usually not yet firmly established. - They are moving towards this skill but have not fully mastered it. *7 months* - By **7 months**, infants have typically refined their grasping skills, including transferring objects from hand to hand and using a **bimanual grip**. - This age is usually past the initial emergence of this specific skill.
Question 3: What is the definition of severe acute malnutrition according to WHO criteria?
- A. Weight for age less than -2 SD
- B. Weight for height less than -2 SD
- C. Weight for age less than -3 SD
- D. Weight for height less than -3 SD (Correct Answer)
Explanation: ***Weight for height less than -3 SD*** - According to the **WHO criteria**, severe acute malnutrition (SAM) is defined by a **weight-for-height Z-score below -3 standard deviations (SD)**. - Other indicators of SAM include a **mid-upper arm circumference (MUAC) less than 115 mm** or the presence of **bilateral pitting edema**. *Weight for age less than -2 SD* - **Weight-for-age below -2 SD** is an indicator of **underweight**, but does not specifically define severe acute malnutrition. - This measure reflects a combination of acute and chronic malnutrition and is insufficient alone to diagnose SAM. *Weight for height less than -2 SD* - **Weight-for-height below -2 SD** signifies **moderate acute malnutrition (MAM)**, not severe acute malnutrition. - This indicates wasting but is not as critical as the -3 SD threshold for SAM. *Weight for age less than -3 SD* - While a low weight-for-age indicates malnutrition, the **-3 SD threshold for weight-for-age** is more indicative of **severe underweight** (a type of chronic malnutrition) rather than specifically severe acute malnutrition, which is primarily characterized by **wasting (low weight-for-height)**. - This measure does not distinguish acute wasting from chronic growth faltering as precisely as weight-for-height.
Question 4: What should be the correct treatment for a 14-year-old child with newly diagnosed Juvenile Rheumatoid Arthritis?
- A. DMARDs with a short course of steroids (Correct Answer)
- B. Only NSAIDs
- C. DMARDs after initial treatment with NSAIDs
- D. Monotherapy with TNF inhibitors
- E. Long-term high-dose corticosteroid therapy
Explanation: ***DMARDs with a short course of steroids*** - For **newly diagnosed rheumatoid arthritis** in children (juvenile idiopathic arthritis), the primary goal is to **control inflammation** and prevent joint damage with **disease-modifying antirheumatic drugs (DMARDs)**. - A **short course of corticosteroids** is often used as a **bridging therapy** to rapidly reduce inflammation while the DMARDs take effect. - This approach ensures **early aggressive treatment** to prevent joint damage while minimizing long-term steroid exposure. *Incorrect: Only NSAIDs* - **NSAIDs** alone provide **symptomatic relief** but do not alter the course of the disease or prevent joint damage in rheumatoid arthritis. - Relying solely on NSAIDs can lead to **progressive joint erosion** and functional impairment. *Incorrect: DMARDs after initial treatment with NSAIDs* - While NSAIDs can be used for initial symptom control, delaying **DMARD initiation** is generally not recommended as it allows for continued joint inflammation and potential damage. - Early and aggressive treatment with DMARDs is crucial for **optimizing long-term outcomes** and preserving joint function. *Incorrect: Monotherapy with TNF inhibitors* - **TNF inhibitors** are potent **biologic DMARDs** and are typically considered for patients who have **failed conventional DMARDs** (e.g., methotrexate). - They are not usually the **first-line monotherapy** for treatment-naive rheumatoid arthritis due to their cost, potential side effects, and the availability of other effective options. *Incorrect: Long-term high-dose corticosteroid therapy* - **Prolonged corticosteroid use** at high doses is associated with significant side effects including growth suppression, osteoporosis, increased infection risk, and cushingoid features. - While steroids are useful as **bridging therapy** for a short duration, long-term high-dose use is avoided in pediatric patients whenever possible.
Question 5: Fast breathing in a 6-month-old infant is taken as:
- A. >30 breaths/min
- B. >50 breaths/min (Correct Answer)
- C. >60 breaths/min
- D. >40 breaths/min
Explanation: ***>50 breaths/min*** - For infants aged 2 to 12 months, a respiratory rate of **greater than 50 breaths per minute** is considered consistent with **tachypnea** or fast breathing. - This is an important indicator of respiratory distress, often used in clinical assessment frameworks like the **Integrated Management of Childhood Illness (IMCI)**. *>30 breaths/min* - A respiratory rate of **>30 breaths/min** would be considered fast breathing for an older child or adult, but it is within the normal range for an infant. - Normal respiratory rates are **higher in infants** and gradually decrease with age. *>60 breaths/min* - While a respiratory rate of **>60 breaths/min** is indeed fast and indicates severe respiratory distress, it is not the initial threshold for defining fast breathing in a 6-month-old infant. - This rate would suggest a more **severe clinical presentation** than simply "fast breathing." *>40 breaths/min* - A respiratory rate **>40 breaths/min** is typically considered fast breathing for children aged 1 to 5 years, but not for infants under 12 months. - For a 6-month-old, this rate is still within the **normal or upper-normal range**, depending on activity and state.
Question 6: Which among the following is NOT part of the classic clinical triad of necrotizing enterocolitis?
- A. Bloody stools
- B. Metabolic acidosis (Correct Answer)
- C. Pneumatosis intestinalis
- D. Abdominal distension
Explanation: ***Metabolic acidosis*** - Metabolic acidosis is **not** part of the classic clinical triad of necrotizing enterocolitis, though it is a common laboratory finding in severe cases. - The **classic triad of NEC** consists of: **abdominal distension**, **bloody stools**, and **pneumatosis intestinalis** on radiography. - Metabolic acidosis occurs as a consequence of intestinal ischemia and sepsis but is not included in the defining triad. *Abdominal distension* - **Abdominal distension** is a cardinal clinical feature and part of the classic triad. - Results from intestinal inflammation, ileus, and gas accumulation. *Bloody stools* - **Bloody stools** (grossly bloody or occult blood positive) are part of the classic triad. - Reflect mucosal injury and intestinal necrosis. *Pneumatosis intestinalis* - **Pneumatosis intestinalis** (intramural gas on abdominal X-ray) is the pathognomonic radiological finding in the classic triad. - Indicates gas-forming bacterial invasion of the damaged intestinal wall.
Question 7: Congenital Rubella Syndrome includes all except
- A. SN deafness
- B. Cataract
- C. VSD
- D. Intracerebral hemorrhage (Correct Answer)
Explanation: ***Intracerebral hemorrhage*** - This is not a typical manifestation of **Congenital Rubella Syndrome** (CRS). Symptoms of CRS primarily include sensory, cardiac, and ocular defects, not bleeding into the brain. *SN deafness* - **Sensorineural (SN) deafness** is a very common and characteristic symptom of **Congenital Rubella Syndrome**, often bilateral, due to damage to the organ of Corti. - It is one of the classic triad of manifestations of CRS. *Cataract* - **Cataracts** (clouding of the lens) are a prominent ocular defect in CRS, often leading to significant vision impairment or blindness. - Ocular defects like cataracts and **microphthalmia** are part of the classic clinical picture. *VSD* - **Ventricular Septal Defect (VSD)** is a common cardiac anomaly seen in CRS, caused by rubella virus infection during heart development. - Other common cardiac defects include **Patent Ductus Arteriosus (PDA)** and **Pulmonary Artery Stenosis**.
Question 8: Which of the following is most specific for congenital Rubella syndrome?
- A. Blueberry muffin rash is seen
- B. Triad of CRS are cataract, cardiac defects, sensorineural deafness (Correct Answer)
- C. Infection is most serious in the first trimester of pregnancy
- D. Virus can be isolated up to 12 months after birth
Explanation: ***Triad of CRS are cataract, cardiac defects, sensorineural deafness*** - The **classic Gregg triad** of **cataracts**, **cardiac defects** (especially patent ductus arteriosus and pulmonary artery stenosis), and **sensorineural deafness** is the **most specific and pathognomonic** feature of **congenital Rubella syndrome**. - While individual components can occur in other conditions, the **combination of this triad** is highly specific for CRS and distinguishes it from other congenital infections. - This triad was first described by **Norman Gregg** in 1941 and remains the hallmark diagnostic feature of congenital rubella syndrome. *Blueberry muffin rash is seen* - The **blueberry muffin rash** (dermal erythropoiesis) presents as purpuric lesions or small dark blue papules and can be seen in congenital rubella syndrome. - However, this finding is **NOT specific to rubella** and occurs in multiple congenital infections including **CMV, toxoplasmosis, parvovirus B19**, and can also be seen in neonatal malignancies like neuroblastoma. - While characteristic, it is less specific than the Gregg triad for diagnosing CRS. *Infection is most serious in the first trimester of pregnancy* - Maternal rubella infection during the **first trimester** carries the highest risk (up to 85% if infected before 12 weeks) of severe multi-organ abnormalities due to rapid organogenesis. - While true, this describes the **timing and severity** of infection rather than a specific clinical feature that distinguishes rubella from other congenital infections. - Many congenital infections (CMV, toxoplasmosis, HSV) are also more severe when acquired in early pregnancy. *Virus can be isolated up to 12 months after birth* - Infants with **congenital Rubella syndrome** can shed virus in bodily fluids (urine, nasopharyngeal secretions) for **12 months or longer** after birth. - This prolonged viral shedding is important for **infection control** and isolation precautions but is a virological characteristic rather than a specific diagnostic clinical feature. - Other congenital infections (CMV) can also demonstrate prolonged viral shedding in infants.
Question 9: Bilateral grasp is seen at what age?
- A. 6 months
- B. 3 months
- C. 9 months
- D. 5 months (Correct Answer)
Explanation: ***5 months*** - At **5 months**, infants typically develop the ability to **reach for and grasp objects with both hands**, demonstrating improved coordination and control. - This age marks a transition from reflexive grasping to more intentional and bilateral manipulation of objects. *6 months* - While fine motor skills continue to develop at 6 months, **bilateral grasp** is usually well-established by this age, having emerged earlier. - At 6 months, infants are often progressing towards **unilateral grasp** and transferring objects between hands. *3 months* - At **3 months**, infants are typically still developing head control and beginning to reach, but their grasp is often still a **reflexive palmar grasp** rather than intentional bilateral grasping. - Reaching at this age is usually more swiping or batting at objects rather than a coordinated grasp. *9 months* - By **9 months**, infants have developed more refined pincer grasp and are capable of complex manipulation of objects with a single hand. - **Bilateral grasp** is a much earlier developmental milestone than the advanced skills seen at 9 months.
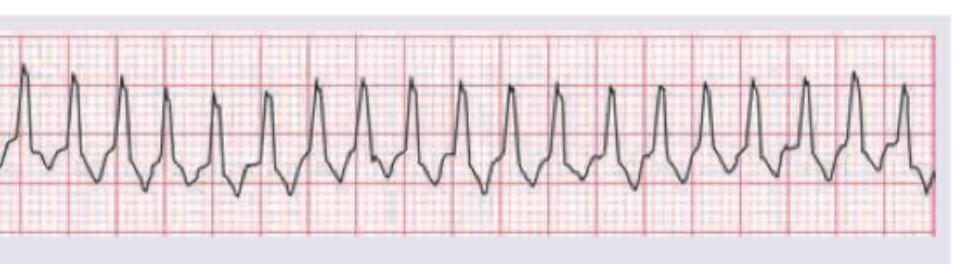
Question 10: Comment on the diagnosis of the patient?
- A. Ventricular tachycardia
- B. Ventricular fibrillation
- C. Electromechanical dissociation
- D. Ventricular flutter (Correct Answer)
Explanation: ***Ventricular flutter*** - This ECG shows a very rapid, regular ventricular rhythm with **sine-wave-like morphology** and no discernible P waves or T waves, characteristic of ventricular flutter. - The rate is typically between **250-350 bpm**, and the QRS complexes are wide and uniform but merge with the T waves to create a continuous undulating pattern. *Ventricular tachycardia* - While ventricular tachycardia (VT) is a fast ventricular rhythm, it usually presents with **discrete QRS complexes** and identifiable (although wide) QRS and ST-T segments. - The rate in VT is typically **100-250 bpm**, and the complexes often show some degree of variability in morphology or R-R interval. *Ventricular fibrillation* - Ventricular fibrillation (VF) is characterized by **chaotic, irregular electrical activity** with no identifiable QRS complexes, P waves, or T waves. - The waveforms are highly variable in shape and amplitude, representing uncoordinated ventricular muscle activity, unlike the regular, undulating pattern seen here. *Electromechanical dissociation* - **Electromechanical dissociation (EMD)**, also known as pulseless electrical activity (PEA), occurs when there is organized electrical activity on the ECG but no palpable pulse. - The ECG in EMD can show a variety of rhythms, including normal sinus rhythm or bradycardia, but it will always show **discernible electrical complexes**, unlike the continuous sinusoidal pattern of ventricular flutter.