All (314)Anatomy (1)Anatomy (26)Anesthesiology (9)Biochemistry (26)Community Medicine (10)Dermatology (15)ENT (7)Forensic Medicine (5)General Medicine (1)Internal Medicine (36)Microbiology (23)Obstetrics and Gynecology (13)Ophthalmology (10)Orthopaedics (6)Pathology (1)Pathology (25)Pediatrics (13)Pharmacology (37)Physiology (15)Psychiatry (2)Psychiatry (4)Radiology (11)Surgery (18)
Q271
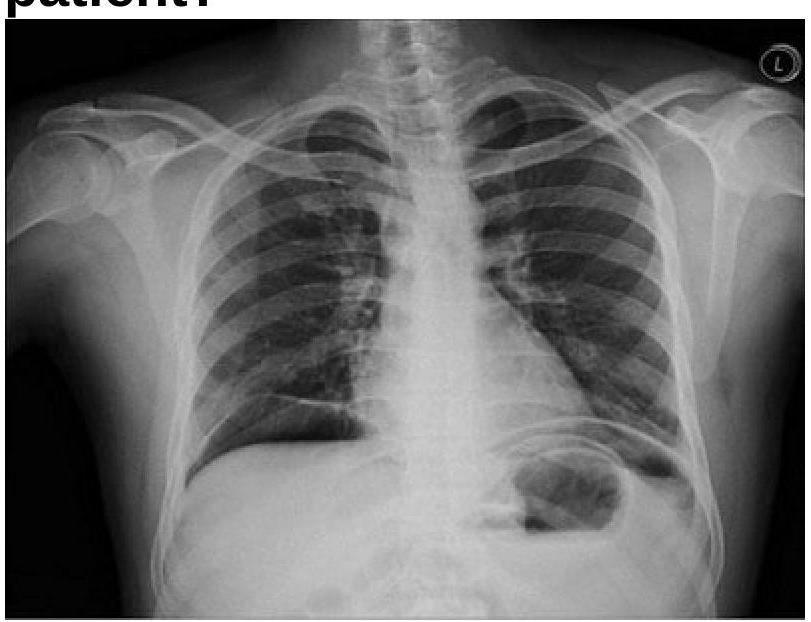
A 40 years old male was brought emergency with severe abdominal pain. On examination, pulse rate was 112/minute and systolic BP was 80 mmHg. Chest x-ray is given below. What is the most appropriate management?