Which of the following is a risk factor for Alzheimer's disease?
Which murmur increases on standing?
A child with history of fever, photosensitivity, rash sparing nasolabial fold presents to OP. Identify the condition?
A 25-year-old female presented to ER unconscious. Her mother tells you about her having recurrent syncopal episodes. Her BP is 80/60 mm Hg and you order an ECG. Treatment is

Polyuria in adults is commonly defined as urine output exceeding:
Patient with ascending paralysis, areflexia and sphincter sparing is seen in?
Not an AIDS defining illness?
Which of the following is not an AIDS defining illness?
Which of the following is the best treatment for refractory ITP?
A patient with rheumatoid arthritis on Methotrexate, steroids and NSAIDs for past 4 months has had no retardation of disease progression. What is the next rational step in management?
NEET-PG 2019 - Internal Medicine NEET-PG Practice Questions and MCQs
Question 21: Which of the following is a risk factor for Alzheimer's disease?
- A. Low blood pressure
- B. Klinefelter syndrome
- C. Down’s syndrome (Correct Answer)
- D. None of the options
Explanation: ***Down’s syndrome*** - Individuals with **Down's syndrome** have an extra copy of chromosome 21, which carries the **amyloid precursor protein (APP) gene**. - This **triplication of the APP gene** leads to increased production of **beta-amyloid protein**, a key component of the plaques found in Alzheimer's disease [1]. *Klinefelter syndrome* - **Klinefelter syndrome** is a genetic condition characterized by an extra X chromosome (XXY), primarily affecting males. - While it can be associated with various health issues, it is **not a known risk factor** for Alzheimer's disease. *Low blood pressure* - **Low blood pressure** (hypotension) is generally not considered a direct risk factor for Alzheimer's disease. - In fact, some studies suggest that **midlife hypertension** (high blood pressure) is a risk factor for later cognitive decline and Alzheimer's. *None of the options* - This option is incorrect because **Down's syndrome** is a well-established and significant risk factor for Alzheimer's disease due to the genetic link involving the APP gene.
Question 22: Which murmur increases on standing?
- A. HOCM (Correct Answer)
- B. MR
- C. MS
- D. VSD
Explanation: ***HOCM*** - Standing decreases **venous return** and **left ventricular volume**, which reduces the size of the LV outflow tract and thus exacerbates the obstruction in **hypertrophic obstructive cardiomyopathy (HOCM)**, making the murmur louder [1]. - This maneuver is a key diagnostic feature as reduced preload intensifies the dynamic obstruction. *MR* - **Mitral regurgitation (MR)** is typically a volume overload lesion, and standing (which reduces preload) generally causes the murmur to **decrease** in intensity due to less blood volume ejected back into the atrium [3]. - The murmur of MR is usually a holosystolic murmur radiating to the axilla [3]. *MS* - **Mitral stenosis (MS)** is a fixed obstruction to left ventricular filling. Changes in preload (like standing) do not significantly alter the gradient across the mitral valve or the intensity of the murmur [2]. - Its characteristic murmur is a **mid-diastolic rumble** with an opening snap [1]. *VSD* - A **ventricular septal defect (VSD)** murmur is caused by blood flowing from the high-pressure left ventricle to the low-pressure right ventricle. Standing, by reducing systemic vascular resistance, would typically cause the murmur to **decrease** in intensity as less blood shunts left-to-right. - The murmur is usually a **holosystolic murmur** best heard at the lower left sternal border.
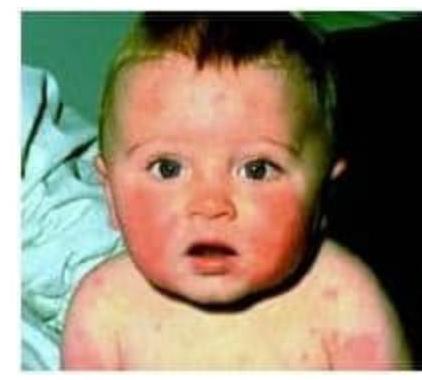
Question 23: A child with history of fever, photosensitivity, rash sparing nasolabial fold presents to OP. Identify the condition?
- A. SLE (Correct Answer)
- B. Polymorphous light eruption
- C. Discoid lupus
- D. Skin tuberculosis
Explanation: ***SLE*** - The combination of **fever**, **photosensitivity**, and a **rash sparing the nasolabial folds** (malar rash or butterfly rash) is highly characteristic of Systemic Lupus Erythematosus (SLE). - Childhood-onset SLE can present with similar mucocutaneous and systemic features as adult-onset disease. *Polymorphous light eruption* - This condition is primarily characterized by **photosensitive skin lesions** but typically does not involve systemic symptoms like fever. - While it presents with rash in sun-exposed areas, it generally lacks the distinct malar rash appearance and systemic involvement seen in SLE. *Discoid lupus* - Discoid lupus is a form of **cutaneous lupus** characterized by chronic, scaly, disfiguring plaques, often on the face and scalp. - It usually **lacks systemic symptoms** like fever and does not present as a widespread malar rash sparing nasal folds. *Skin tuberculosis* - Skin tuberculosis (lupus vulgaris or scrofuloderma) presents with **nodular, plaque-like lesions** or cold abscesses, often with ulceration and scarring. - It is not typically associated with **photosensitivity** or a malar rash, and fever, if present, is usually due to systemic Mycobacterium infection.
Question 24: A 25-year-old female presented to ER unconscious. Her mother tells you about her having recurrent syncopal episodes. Her BP is 80/60 mm Hg and you order an ECG. Treatment is
- A. Cathether Ablation
- B. Adenosine
- C. DC shock (Correct Answer)
- D. Radiofrequency ablation
Explanation: ***DC shock*** - The ECG shows a **wide complex tachycardia** with alternating morphology in the QRS complex, consistent with **Torsades de Pointes**. - Given the patient's **unconsciousness** and **hypotension (80/60 mmHg)**, she is hemodynamically unstable, making immediate **electrical cardioversion (DC shock)** the treatment of choice irrespective of the cause. *Catheter Ablation* - **Catheter ablation** is an invasive procedure used for definitive treatment of recurrent arrhythmias, often considered in patients who are *hemodynamically stable*. - It is not an acute, emergency treatment for an **unstable patient** in a life-threatening arrhythmia. *Adenosine* - **Adenosine** is primarily used to terminate **supraventricular tachycardias (SVTs)** and can be harmful in wide complex tachycardias, especially if due to ventricular tachycardia or Wolff-Parkinson-White syndrome. - Its use is contraindicated in wide complex tachycardias like Torsades de Pointes, and it would not be effective in an **unstable patient** with Torsades de Pointes. *Radiofrequency ablation* - **Radiofrequency ablation** is a type of catheter ablation, which ablates or destroys abnormal electrical pathways in the heart. - Similar to other ablative therapies, it is a **definitive treatment** for recurrent arrhythmias in *stable patients*, not an emergency measure for an unconscious, hypotensive patient with an acute arrhythmia.
Question 25: Polyuria in adults is commonly defined as urine output exceeding:
- A. 50 ml/ kg / day
- B. 30 ml / Kg/ day
- C. 60 ml/ kg / day
- D. 40 ml / Kg/ day (Correct Answer)
Explanation: ***40 ml / Kg/ day*** - **Polyuria** is clinically defined as urine output exceeding 3 liters per 24 hours (L/day) in adults. - Converting this to a weight-based measurement for an average 75 kg adult, 3 L/day equates to approximately **40 ml/kg/day**. *50 ml/ kg / day* - This value represents a significantly higher urine output than the standard clinical definition of **polyuria**, making it an unlikely threshold. - While excessive, it would indicate a more severe and less common degree of diuresis, not the general definition. *30 ml / Kg/ day* - This value is below the typical threshold for **polyuria** and is closer to what might be considered normal or slightly elevated urine output. - Normal urine output is typically between **0.5-1 ml/kg/hour**, which translates to 12-24 ml/kg/day. *60 ml/ kg / day* - This is a substantially high urine output, indicating a profound level of **diuresis**, well beyond the standard definition of polyuria. - While possible in extreme cases, it is not the common cutoff used for defining polyuria.
Question 26: Patient with ascending paralysis, areflexia and sphincter sparing is seen in?
- A. G.B.S (Correct Answer)
- B. Botulinism
- C. Snake bite
- D. Polio
Explanation: **G.B.S** - **Guillain-Barré Syndrome (GBS)** is characterized by **ascending paralysis** and **areflexia**, meaning loss of deep tendon reflexes [1]. - **Sphincter sparing** is also typical in GBS, differentiating it from other causes of paralysis where autonomic involvement can lead to bladder and bowel dysfunction [1]. *Botulism* - Botulism typically presents with **descending paralysis**, weakness starting in the cranial nerves and progressing downwards. - While it causes significant muscle weakness and can lead to **areflexia**, the pattern of paralysis (descending vs. ascending) and the presence of prominent cranial nerve involvement help distinguish it. *Snake bite* - Neurotoxic snake bites can cause **flaccid paralysis** and **areflexia**, but the paralysis often starts at the site of the bite or affects cranial nerves preferentially before generalized ascending paralysis. - The history of a **snake bite** and presence of **local envenomation signs** (swelling, pain) would also be prominent. *Polio* - Polio primarily causes **asymmetric flaccid paralysis** and **areflexia**, due to the destruction of anterior horn cells in the spinal cord. - Unlike GBS, polio does not typically present with an ascending pattern affecting both sides symmetrically and often involves sensory sparing.
Question 27: Not an AIDS defining illness?
- A. Progressive multifocal leukoencephalopathy
- B. Lymphoma of brain < 60 years of age
- C. Extrapulmonary Cryptococcosis
- D. Tertiary Syphilis (Correct Answer)
Explanation: ***Tertiary Syphilis*** - While a serious late-stage manifestation of **syphilis**, it is not specifically listed as an **AIDS-defining illness** by the CDC, although HIV-positive individuals may be more susceptible to its complications [1]. - **Neurosyphilis**, a form of tertiary syphilis affecting the central nervous system, is also not an AIDS-defining condition on its own, unlike some other opportunistic infections [1]. *Progressive multifocal leukoencephalopathy (PML)* - PML, caused by the **JC virus**, is an **AIDS-defining illness** characterized by the progressive destruction of myelin in the brain, leading to severe neurological deficits. - It occurs almost exclusively in individuals with severe **immunodeficiency**, such as those with untreated HIV infection. *Lymphoma of brain < 60 years of age* - **Primary central nervous system (CNS) lymphoma** in individuals with HIV, especially those under 60 years of age, is an **AIDS-defining condition** [2]. - Its occurrence is strongly linked to severe immunosuppression in HIV-infected patients [2]. *Extrapulmonary Cryptococcosis* - **Cryptococcosis**, when it affects sites outside the lungs (e.g., **cryptococcal meningitis**), is an **AIDS-defining illness**. - This fungal infection is a common opportunistic infection in individuals with advanced HIV disease.
Question 28: Which of the following is not an AIDS defining illness?
- A. Cervical cancer
- B. Hodgkin's lymphoma (Correct Answer)
- C. Primary CNS lymphoma
- D. Kaposi sarcoma
Explanation: ***Hodgkin's lymphoma*** - While patients with HIV are at an increased risk of developing **Hodgkin's lymphoma**, it is not officially classified as an **AIDS-defining illness** by the CDC [3]. - AIDS-defining conditions primarily include certain opportunistic infections and specific malignancies [4]. *Cervical cancer* - **Invasive cervical cancer** is an AIDS-defining illness in HIV-positive women, indicating severe immunosuppression [4]. - This is because HIV infection can accelerate or worsen the progression of **HPV-related cervical dysplasia** to invasive cancer [4]. *Primary CNS lymphoma* - **Primary CNS lymphoma** (brain lymphoma) is an AIDS-defining illness, particularly when associated with **Epstein-Barr virus** [2]. - Its presence indicates a significant degree of **immunodeficiency** in HIV-infected individuals. *Kaposi sarcoma* - **Kaposi sarcoma** is a well-known and common AIDS-defining malignancy, caused by **Human Herpesvirus 8 (HHV-8)** [1]. - It presents as vascular lesions on the skin, mucous membranes, internal organs, and lymph nodes [1].
Question 29: Which of the following is the best treatment for refractory ITP?
- A. Platelet transfusion
- B. Azathioprine
- C. Prednisolone
- D. Splenectomy (Correct Answer)
Explanation: ***Splenectomy*** - **Splenectomy** is considered the most effective treatment for **refractory immune thrombocytopenic purpura (ITP)**, especially in patients who have failed multiple lines of medical therapy [1]. - The spleen is the primary site of **platelet destruction** and **antibody production** against platelets in ITP, so its removal can lead to a sustained increase in platelet count [1]. *Platelet transfusion* - While platelet transfusions can temporarily increase platelet counts, they are generally reserved for **acute, life-threatening bleeding** in ITP, not as a definitive treatment for refractory cases. - Transfused platelets are rapidly destroyed by the same **autoantibodies** that target endogenous platelets, making their effect short-lived. *Azathioprine* - **Azathioprine** is an **immunosuppressant** that can be used in ITP, but it is typically a **second-line** or **third-line agent** and its response takes time [1]. - It is not considered the "best" treatment for refractory ITP compared to splenectomy, which offers a more immediate and often sustained response [1]. *Prednisolone* - **Prednisolone** (corticosteroids) is often the **first-line treatment** for ITP due to its rapid immunosuppressive effects. - However, for **refractory ITP** (meaning it has not responded adequately to initial treatments), corticosteroids alone are usually insufficient to achieve long-term remission [1].
Question 30: A patient with rheumatoid arthritis on Methotrexate, steroids and NSAIDs for past 4 months has had no retardation of disease progression. What is the next rational step in management?
- A. Continue Methotrexate and steroids at higher dose
- B. Stop oral Methotrexate and start parenteral Methotrexate
- C. Add Sulfasalazine (Correct Answer)
- D. Start treatment with anti-TNF alpha drugs
Explanation: Focus on **Add Sulfasalazine**: - Since the patient has not responded to **Methotrexate** alone, adding a second conventional synthetic **disease-modifying antirheumatic drug (DMARD)** like **Sulfasalazine** is a common and appropriate step in a **treat-to-target strategy** for rheumatoid arthritis [1]. - This approach aims to achieve **disease remission** or **low disease activity** by combining therapies to enhance efficacy. *Continue Methotrexate and steroids at higher dose* - Increasing the dose of **Methotrexate** might be considered if the current dose is sub-optimal, but after 4 months with no improvement, simply continuing current medications at higher doses without adding another agent is less likely to significantly alter **disease progression** [1]. - Prolonged higher-dose **steroids** carry significant risks and are generally used for symptom control, not primary disease modification. *Stop oral Methotrexate and start parenteral Methotrexate* - Switching to **parenteral Methotrexate** is considered if **oral Methotrexate** absorption is an issue or if the patient experiences gastrointestinal side effects [1]. - While parenteral administration can improve bioavailability, it doesn't represent a change in therapeutic strategy for **uncontrolled disease activity**. *Start treatment with anti-TNF alpha drugs* - **Biologic DMARDs** like **anti-TNF alpha drugs** are typically reserved for patients who have failed **two or more conventional synthetic DMARDs**, including **Methotrexate**, or in cases of severe, rapidly progressing disease [2]. - While effective, they are more expensive and have different side effect profiles, making them a later-line treatment in the management algorithm [2].